Causes of Shoulder Pain in Females: Full 2026 Guide
The causes of shoulder pain in females span musculoskeletal injury, hormonal shifts, autoimmune disease, postural dysfunction, and referred pain from internal organs including the heart. Women experience several shoulder conditions at significantly higher rates than men, and the biological reasons for that difference are specific, clinically established, and rarely explained in general health content.
According to the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), frozen shoulder affects women at roughly twice the rate it affects men, and rotator cuff conditions are increasingly recognized as having sex-differentiated presentations tied to hormonal exposure and anatomical variation. These are not coincidental patterns. They reflect real differences in tendon biology, joint capsule composition, and inflammatory signaling that change across a woman’s reproductive lifespan.
This article covers every major cause of shoulder pain specific to female physiology, the named biological mechanisms behind each one, the life stages at which each cause is most common, and the specific situations in which shoulder pain in a woman warrants immediate emergency evaluation rather than a wait-and-see approach.
Causes of Shoulder Pain in Female: An Overview
The causes of shoulder pain in females fall into five broad categories: structural and mechanical injury, hormonal and endocrine-related conditions, autoimmune and inflammatory disease, referred pain from visceral organs, and postural or occupational factors.
Not every cause is unique to women. But the frequency, timing, and physiological drivers behind several common shoulder conditions differ meaningfully between biological sexes. A 45-year-old woman with progressively stiffening shoulder pain is facing a very different clinical picture than a 45-year-old man with the same complaint, even if the anatomical location of the pain is identical.
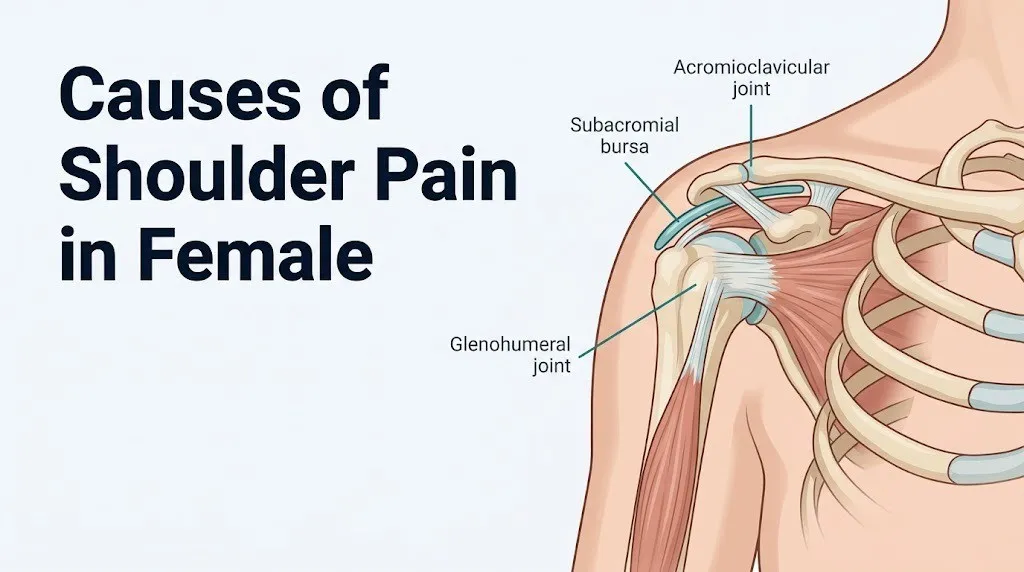
The glenohumeral joint (the main ball-and-socket joint of the shoulder, formed by the humeral head articulating with the glenoid fossa of the scapula) is the most mobile joint in the human body. That mobility comes at the cost of inherent stability. Four muscles, collectively called the rotator cuff (supraspinatus, infraspinatus, teres minor, subscapularis), stabilize the joint actively. Ligaments, the joint capsule, and the fibrocartilaginous labrum provide passive stability. Any disruption to these structures, whether from injury, degeneration, inflammation, or systemic disease, can produce shoulder pain.
The shoulder also sits at the convergence of several neural pathways. The phrenic nerve, which originates from cervical nerve roots C3, C4, and C5, passes alongside the heart and diaphragm before reaching its target organ. This anatomical proximity means that irritation of the diaphragm or heart can produce pain perceived as coming from the shoulder or neck, a mechanism critical to understanding why left shoulder pain in women warrants cardiac evaluation.
| Cause Category | Most Common Example | Female-Specific Risk? | Peak Age Group |
|---|---|---|---|
| Structural/mechanical | Rotator cuff tendinopathy | Moderate | 40-60 |
| Hormonal/endocrine | Frozen shoulder (adhesive capsulitis) | High | 40-60 |
| Autoimmune/inflammatory | Rheumatoid arthritis shoulder | High | 30-60 |
| Referred/visceral | Cardiac ischemia (left shoulder) | High for atypical MI | 50+ |
| Postural/occupational | Subacromial impingement | Moderate | 30-55 |
| Pregnancy-related | Relaxin-mediated joint laxity | Female-specific | Reproductive age |
Why Women Are More Prone to Shoulder Pain Than Men
Women experience certain shoulder conditions at disproportionately higher rates than men because of real, named differences in joint anatomy, hormonal biology, and connective tissue physiology.
Research published in the Journal of Shoulder and Elbow Surgery has found that women have a smaller subacromial space (the gap between the top of the humeral head and the undersurface of the acromion through which the supraspinatus tendon passes) than men on average. A narrower subacromial space means the supraspinatus tendon is more likely to be compressed during overhead movements, increasing the risk of subacromial impingement syndrome and rotator cuff tendinopathy.
Connective tissue composition also differs by biological sex. Estrogen receptors are present on tendon fibroblasts, the cells responsible for producing and maintaining collagen in tendons and ligaments. When estrogen levels are physiologically normal, this receptor activity supports collagen cross-linking and tensile strength. When estrogen levels decline, as occurs in perimenopause and postmenopause, collagen synthesis slows and tendon integrity degrades more rapidly. This is not a minor effect. A 2021 study in Arthritis and Rheumatology found that postmenopausal women had measurably reduced tendon stiffness compared to premenopausal women of similar activity levels, a difference not replicated in men of comparable age.
Women are also two to three times more likely than men to develop autoimmune conditions, including rheumatoid arthritis and systemic lupus erythematosus (SLE), both of which affect shoulder joints through immune-mediated synovial inflammation. The biological basis for this sex-biased immune susceptibility includes the immunomodulatory effects of estrogen on B-cell and T-cell activation, as described in research from the National Institutes of Health.
Quick Tip:
- Women with a family history of autoimmune disease are at elevated risk for inflammatory shoulder conditions independent of injury or overuse.
- Women who work in roles involving repeated overhead reaching face a compounded risk due to both anatomical narrowing of the subacromial space and estrogen-related tendon vulnerability as they age.
- Postmenopausal women on no hormone replacement therapy should inform their orthopedic provider, as their tendon healing capacity may differ from premenopausal norms.
Hormonal Influences on Shoulder Pain in Women
Hormonal changes across a woman’s reproductive lifespan directly influence shoulder joint health through multiple named physiological pathways, making hormonal status one of the most important and most overlooked factors in evaluating shoulder pain in females.
Estrogen (17-beta-estradiol), produced primarily by the ovarian granulosa cells during reproductive years, acts on estrogen receptors (specifically ERalpha and ERbeta subtypes) present in tendon fibroblasts and synovial tissue. At physiological levels, estrogen promotes collagen type I synthesis, supports tendon elasticity, and suppresses the production of pro-inflammatory cytokines including interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-alpha). This is why many women experience a transient increase in musculoskeletal discomfort during the low-estrogen phase of their menstrual cycle, just before menstruation begins.
Progesterone has a secondary effect on joint laxity. At higher concentrations during the luteal phase of the menstrual cycle, progesterone mildly increases ligament compliance. Over years of cycling, this cyclical laxity may contribute incrementally to micro-instability at the glenohumeral joint, which can predispose to labral wear and anterior shoulder instability, particularly in women who perform repetitive overhead activities.
Thyroid hormones present a clinically underrecognized pathway. Hypothyroidism, which affects women at approximately seven times the rate it affects men according to the American Thyroid Association, causes reduced collagen turnover, myxedematous tissue deposits in joint capsules, and altered synovial fluid composition. This combination produces a stiffening process in the glenohumeral joint capsule that closely mimics the early stages of frozen shoulder. Women being evaluated for adhesive capsulitis should routinely have thyroid function assessed, as undiagnosed hypothyroidism is a correctable contributing cause.
- Estrogen decline in perimenopause: increases tendon degeneration risk, raises inflammatory cytokine levels in joint tissue
- Cyclical progesterone: mildly increases glenohumeral ligament laxity during luteal phase
- Hypothyroidism (TSH elevated, free T4 low): produces capsular stiffening mimicking early frozen shoulder
- Diabetes mellitus (more prevalent in women with PCOS): strongly associated with adhesive capsulitis development, with a 3-5x higher risk compared to nondiabetic women per AAOS data
Key Takeaway: Hormonal status, especially estrogen decline and undiagnosed hypothyroidism, is a direct and biologically specific driver of several common shoulder conditions in women, not merely a background factor.
Frozen Shoulder in Women: Causes and Mechanisms
Frozen shoulder, clinically termed adhesive capsulitis, is one of the most female-predominant shoulder conditions in clinical medicine, affecting women at approximately twice the rate of men, with peak incidence between ages 40 and 60.
Adhesive capsulitis occurs when the glenohumeral joint capsule undergoes inflammatory fibroblastic proliferation, meaning that fibroblasts (connective tissue cells) multiply abnormally within the joint capsule and produce excessive collagen. That excess collagen forms scar-like adhesions, reduces the volume of synovial fluid within the joint space, and physically contracts the capsule. The result is a shoulder that becomes progressively more painful, then progressively more restricted in every direction of movement. Think of it like a rubber glove shrinking around your hand while simultaneously becoming less pliable. The joint does not lock from the outside. It constricts from within.
According to the American Academy of Orthopaedic Surgeons (AAOS), adhesive capsulitis typically progresses through three stages: the freezing stage (progressive pain and early stiffness, lasting 2 to 9 months), the frozen stage (pain may decrease but stiffness becomes maximal, lasting 4 to 12 months), and the thawing stage (gradual recovery of range of motion, lasting 5 to 24 months). Many women present for evaluation during the frozen stage, when stiffness has become debilitating but the acute pain of the early inflammatory stage has partially subsided.
Estrogen receptors on glenohumeral joint capsule fibroblasts are believed to modulate this fibrotic process. Preliminary research published in the Journal of Shoulder and Elbow Surgery suggests that declining estrogen levels reduce the anti-fibrotic influence on capsular fibroblasts, allowing unchecked proliferation. This mechanism, while still under active investigation, explains in part why adhesive capsulitis clusters around perimenopause.
Women with diabetes mellitus face a three to five times higher risk of developing frozen shoulder compared to nondiabetic women. The mechanism involves advanced glycation end-products (AGEs) binding to collagen in the joint capsule, making it stiffer and more prone to fibrotic change. Women with type 2 diabetes or polycystic ovary syndrome (PCOS) with insulin resistance should be monitored for early shoulder stiffness symptoms.
Rotator Cuff Problems as a Cause of Shoulder Pain in Females
Rotator cuff pathology, ranging from rotator cuff tendinopathy (overuse-related tendon degeneration without full-thickness tear) to partial and complete rotator cuff tears, is among the most frequent structural causes of shoulder pain across all adults, but several aspects of its presentation and progression differ meaningfully in women.
The rotator cuff is a four-muscle group: the supraspinatus (primarily responsible for initiating shoulder abduction), the infraspinatus and teres minor (responsible for external rotation), and the subscapularis (responsible for internal rotation). The supraspinatus tendon is the most commonly injured of the four. It passes through the subacromial space, a narrow anatomical corridor beneath the acromion (the bony prominence at the top of the shoulder). Repeated overhead movement, or structural narrowing of this space, causes the tendon to be mechanically compressed with each arm elevation. Over time, this compression produces microtearing, localized prostaglandin-mediated inflammation, and tendon degeneration.
According to a study published in JAMA Internal Medicine reviewing imaging data across age groups, the prevalence of full-thickness rotator cuff tears increases sharply with age, from approximately 4% in adults under 40 to over 50% in adults over 80. Women have a higher rate of supraspinatus tendon degeneration in the 50 to 65 age range than men of comparable physical activity levels, a difference attributed in part to estrogen-related changes in tendon collagen composition during the postmenopausal transition.
A partial rotator cuff tear typically produces pain that is worse with overhead activities (reaching above the shoulder, lifting away from the body), pain at night when lying on the affected shoulder, and a characteristic arc of pain between 60 and 120 degrees of shoulder elevation. A complete tear may produce profound weakness with attempted arm elevation, though not always severe pain in the acute phase.
Women who present with rotator cuff symptoms should have their evaluation include an assessment of thyroid function and metabolic status, since both hypothyroidism and diabetes alter tendon healing and can convert manageable tendinopathy into a more severe degenerative pattern without appropriate treatment.
Shoulder Bursitis in Women: What Causes It
Shoulder bursitis refers to inflammation of the subacromial bursa, a fluid-filled sac positioned between the supraspinatus tendon and the undersurface of the acromion. Its job is to reduce friction as the rotator cuff tendons slide beneath the acromion during arm movement. When the bursa becomes inflamed, that friction reduction disappears and arm movement becomes painful.
The most common mechanism is repetitive mechanical irritation. Repeated overhead reaching, lifting, or throwing compresses the bursa against the acromion. Over time, the bursal lining (the synovium) becomes inflamed, the bursa fills with excess fluid, and the space available for pain-free tendon movement narrows further. Prostaglandins produced by the inflamed synovium sensitize local pain receptors, producing a characteristic aching pain that typically worsens with arm elevation and sometimes disturbs sleep.
The Centers for Disease Control and Prevention notes that occupational musculoskeletal injuries disproportionately affect women in healthcare, food service, and manufacturing roles, industries with high rates of repetitive overhead or forward-reaching work. Women in these occupations develop shoulder bursitis at rates that reflect cumulative mechanical loading over years rather than a single acute event.
Subacromial bursitis in women can also develop secondary to other shoulder conditions. When rotator cuff tendinopathy is present, the tendon thickens with degeneration, further reducing subacromial space and compressing the bursa even without repetitive overhead work. This combined pathology (tendinopathy plus secondary bursitis) is common in women over 45 and is one reason why shoulder pain in this age group often involves multiple overlapping structures rather than a single isolated diagnosis.
Women with inflammatory arthritis (rheumatoid arthritis, psoriatic arthritis, gout) can develop bursal inflammation through a different mechanism: systemic inflammatory mediators including IL-6 and TNF-alpha travel through the bloodstream and produce synovitis within the bursa directly, without any mechanical trigger.
Key Takeaway: Shoulder bursitis in women is most commonly driven by cumulative mechanical loading or secondary inflammation from rotator cuff degeneration, and in women over 45, these two processes frequently coexist in the same shoulder.
Acromioclavicular Joint Pain in Females
The acromioclavicular (AC) joint, the connection between the acromion (part of the scapula) and the outer end of the clavicle (collarbone), is a frequent source of shoulder pain that often goes undiagnosed because it produces a distinct but easily missed pattern: pain located specifically at the very top of the shoulder, not deep inside it.
AC joint pain in women typically arises from two sources. The first is direct trauma, such as a fall onto an outstretched arm or a blow to the top of the shoulder, which can sprain or disrupt the acromioclavicular ligaments. The second is AC joint osteoarthritis, a degenerative process in which the fibrocartilage disc within the AC joint gradually wears down, bony osteophytes (spurs) form at the joint margins, and the joint space narrows. AC joint osteoarthritis is common in middle-aged and older women and frequently coexists with rotator cuff pathology.
Because the AC joint sits directly at the top of the shoulder, pain from this source often worsens specifically when the arm is brought across the body (adduction), such as when reaching across a table to the opposite side, or when lying on the affected shoulder. This cross-body pain pattern differentiates AC joint pain from purely rotator cuff or bursal sources, which are more typically aggravated by overhead elevation.
Hormonal factors influence AC joint health similarly to other shoulder structures. The acromioclavicular ligaments contain estrogen receptors, and postmenopausal ligament laxity combined with reduced articular cartilage maintenance accelerates AC joint degeneration in women who are no longer producing endogenous estrogen.
Women who perform repeated cross-body arm movements in work or sport settings (assembly line workers, swimmers, tennis players) face an elevated cumulative load on the AC joint and should be evaluated specifically for AC joint pathology as a distinct source when presenting with top-of-shoulder pain.
Shoulder Pain During Pregnancy
Shoulder pain during pregnancy is a female-specific cause driven primarily by the hormonal, postural, and circulatory changes that accompany pregnancy, though one presentation during pregnancy warrants immediate emergency evaluation.
Relaxin, a hormone produced by the corpus luteum from early pregnancy and later by the placenta, increases throughout the first trimester and peaks around 12 weeks. According to the American College of Obstetricians and Gynecologists (ACOG), relaxin acts on receptors in ligamentous tissue throughout the body to increase collagen degradation and reduce connective tissue stiffness. In the pelvis, this prepares the body for delivery. But relaxin acts systemically, not selectively. The coracohumeral ligament and the glenohumeral joint capsule also respond to relaxin, producing measurable increases in glenohumeral joint laxity. In women with pre-existing shoulder instability or a history of shoulder dislocation, this hormonally driven laxity can worsen symptoms or precipitate new instability episodes.
Postural changes in pregnancy, particularly the anterior shifting of the center of gravity as the uterus enlarges, cause compensatory changes in thoracic and lumbar spine curvature. These postural adaptations frequently produce a rounded-shoulder posture, which alters the mechanics of the acromioclavicular joint and subacromial space and can trigger or worsen subacromial impingement pain.
Shoulder pain in late pregnancy or the early postpartum period that occurs alongside swelling, elevated blood pressure, or visual changes requires immediate evaluation. These symptoms may indicate preeclampsia or, more acutely, HELLP syndrome (Hemolysis, Elevated Liver enzymes, Low Platelet count), in which right shoulder or right upper abdominal pain can occur due to hepatic capsule distension and referred pain through the diaphragm via the phrenic nerve. This is a distinct obstetric emergency.
Postpartum shoulder pain is also extremely common due to the biomechanical demands of infant feeding: prolonged static neck flexion, asymmetric arm loading during breastfeeding or bottle-feeding, and carrying the infant in one arm rather than alternating sides. A postpartum woman with unilateral shoulder pain should be evaluated for these postural contributions before assuming a structural cause.
Key Takeaway: Shoulder pain during pregnancy is common and often mechanical, but right shoulder pain accompanied by upper abdominal pain, elevated blood pressure, or swelling during pregnancy is a potential obstetric emergency requiring immediate evaluation.
Postmenopausal Shoulder Pain Causes
The postmenopausal period, defined clinically as the 12 months following the final menstrual period and all subsequent years, represents a significant inflection point in female musculoskeletal health, and the shoulder is one of the most commonly affected joints.
Estrogen withdrawal at menopause removes several protective effects simultaneously. Collagen synthesis in tendons slows. The anti-inflammatory signaling that estrogen provided to shoulder joint tissue is reduced. Fibroblast behavior in the glenohumeral joint capsule shifts toward a pro-fibrotic pattern. Articular cartilage at the acromioclavicular and glenohumeral joints loses a portion of its maintenance signaling. The practical result is that postmenopausal women experience accelerated rates of rotator cuff degeneration, higher rates of frozen shoulder, and greater rates of glenohumeral osteoarthritis than premenopausal women of comparable physical activity levels.
Polymyalgia rheumatica (PMR), an inflammatory condition characterized by bilateral shoulder and hip girdle pain with significant morning stiffness, almost exclusively affects adults over age 60 and affects women at roughly twice the rate of men. According to the American College of Rheumatology (ACR), PMR is associated with markedly elevated inflammatory markers (ESR and CRP) and responds dramatically to low-dose corticosteroid treatment. Women over 60 presenting with bilateral shoulder pain and morning stiffness lasting more than 45 minutes should be specifically evaluated for PMR, as misdiagnosis as degenerative joint disease delays effective treatment.
Bone density loss at menopause, driven by estrogen withdrawal from osteoclast-suppressing activity, also affects the humeral head and acromion. Osteoporotic bone changes can alter the structural integrity of the subacromial space and predispose to stress fractures of the humeral head or clavicle after relatively minor trauma, injuries that can be missed if imaging is not performed.
Women in this age group taking aromatase inhibitors for breast cancer treatment face an amplified form of estrogen withdrawal. Aromatase inhibitors, which suppress the conversion of androgens to estrogen, are associated with joint pain (arthralgias) in approximately 47% of users according to research published in the New England Journal of Medicine. For these women, shoulder pain may be a treatment-related side effect requiring management discussion with their oncologist and primary care physician jointly.
Autoimmune and Inflammatory Causes of Shoulder Pain in Women
Women develop autoimmune conditions at disproportionately high rates compared to men, and several of these conditions produce shoulder pain through named immune-mediated mechanisms that differ fundamentally from mechanical causes.
Rheumatoid arthritis (RA) affects approximately 1.5 million Americans, and roughly 75% of those affected are women, according to the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS). RA is driven by an aberrant immune response in which T-cells and B-cells mistakenly attack synovial tissue, the membrane lining the joints. In the shoulder, this produces synovitis (painful, warm, swollen joint lining), progressive cartilage destruction, and eventual joint deformity if untreated. The inflammatory mediators driving this process include TNF-alpha, IL-6, and IL-1beta, all of which are measurably elevated in RA-affected joint fluid.
Systemic lupus erythematosus (SLE) affects women at approximately nine times the rate of men, with peak incidence in women of childbearing age (15 to 45 years). Lupus-related shoulder pain typically occurs through two mechanisms: lupus arthritis (immune complex deposition in synovial tissue producing joint inflammation) and avascular necrosis of the humeral head (impaired blood supply to the humeral head, often related to corticosteroid treatment for lupus, leading to bone tissue death and structural collapse of the joint). A woman with known lupus who develops new or worsening shoulder pain should have avascular necrosis ruled out before attributing the pain to arthritis flare.
Shoulder joint inflammation in autoimmune conditions is distinguished from mechanical causes by its characteristic bilateral distribution, its association with systemic features (fatigue, fever, rash, morning stiffness lasting more than one hour), and its responsiveness to anti-inflammatory treatment rather than mechanical rest.
- Rheumatoid arthritis: bilateral shoulder synovitis, elevated anti-CCP and rheumatoid factor (RF), responds to disease-modifying antirheumatic drugs (DMARDs)
- Systemic lupus erythematosus: shoulder arthritis or avascular necrosis, associated with ANA positivity, butterfly rash, photosensitivity
- Polymyalgia rheumatica: bilateral shoulder and hip girdle stiffness, exclusively in adults over 50, dramatic corticosteroid response
- Psoriatic arthritis: shoulder involvement with skin or nail psoriasis; seronegative on standard RA markers
Key Takeaway: Autoimmune shoulder conditions are three to nine times more prevalent in women and are identified by bilateral presentation, systemic symptoms, and specific blood markers rather than a history of mechanical injury.
Referred Pain to the Shoulder in Females Including Cardiac Causes
Referred pain to the shoulder, meaning pain perceived at the shoulder that originates from a distant internal structure rather than from the shoulder itself, is one of the most clinically important and most underemphasized causes of shoulder pain in women.
The anatomical basis for referred shoulder pain lies in shared neural pathways. The phrenic nerve, which originates from cervical nerve roots C3, C4, and C5 and carries sensation from the diaphragm, shares dermatomal territory with the skin and tissue of the upper shoulder and neck. When any structure adjacent to the diaphragm or the undersurface of the liver becomes irritated, inflamed, or ischemic, the brain may interpret those pain signals as originating from the shoulder or neck rather than the internal organ. This is referred pain: real pain, neurologically mediated, but anatomically displaced from its true source.
The most medically urgent form of referred shoulder pain in women is pain from myocardial ischemia (heart muscle deprived of adequate blood flow due to coronary artery blockage). The American Heart Association (AHA) has published extensive evidence documenting that women experiencing a heart attack are significantly more likely than men to present with atypical symptoms, including left shoulder pain, jaw pain, nausea, unusual fatigue, and shortness of breath, rather than the classic central crushing chest pressure more commonly described in men. This difference reflects both a higher rate of small-vessel coronary artery disease in women (which produces a diffuse ischemic pattern rather than a focal infarction) and sex-based differences in pain processing pathways.
Gallbladder disease, which affects women at approximately twice the rate of men, can produce right shoulder pain through a similar diaphragmatic referral mechanism. When the gallbladder (located under the right side of the liver) becomes inflamed or distended by a gallstone blockage, it irritates the adjacent right diaphragm, producing referred pain to the right shoulder tip, right upper abdomen, or interscapular region.
Subdiaphragmatic irritation from any cause, including postoperative free air, a ruptured ectopic pregnancy, or a liver abscess, can produce bilateral or unilateral referred shoulder pain. A woman with shoulder pain and any accompanying abdominal, chest, or systemic symptoms should have referred causes ruled out as a clinical priority.
Posture and Repetitive Strain as Causes of Shoulder Pain in Females
Postural dysfunction and cumulative repetitive strain are among the most common and most modifiable causes of shoulder pain in working-age women, driven by a combination of occupational roles, caregiving physical demands, and the seated or static postures that characterize both desk-based work and extended smartphone use.
The shoulder complex depends on the coordinated positioning of three bones: the humerus, the scapula, and the clavicle. When the thoracic spine rounds forward into sustained kyphosis (as occurs during prolonged desk work or forward head posture), the scapula tilts anteriorly and moves away from the thoracic wall. This scapular malposition, called scapular dyskinesis, reduces the functional subacromial space and changes the mechanical advantage of the rotator cuff muscles. Think of it like trying to open a door when the hinges are bent. The mechanism works, but with increased friction and abnormal stress at every point of load.
Women in sedentary work roles, particularly those working at computer stations without ergonomic shoulder support, demonstrate significantly higher rates of neck and shoulder girdle musculature fatigue (upper trapezius, levator scapulae, serratus anterior) than men in comparable roles. Research published in Occupational and Environmental Medicine has attributed this partly to women’s lower absolute muscle mass in the shoulder girdle, meaning their muscles reach a proportionally higher percentage of maximal voluntary contraction during identical tasks compared to men doing the same work.
Women who are primary caregivers, whether for infants, children, or elderly family members, face a second category of repetitive strain. Repeated lifting, carrying, and positioning of another person places asymmetric and cumulative loads on the shoulder joint, particularly when carrying is done predominantly on one side.
To describe postural shoulder pain to your doctor effectively:
- Note which specific movements make the pain worse: overhead, cross-body, behind the back, or at rest.
- Note the time of day when pain is worst: morning stiffness (autoimmune pattern) versus end-of-workday worsening (mechanical fatigue pattern).
- Note any relationship to specific activities: computer use, infant feeding, driving, or sleeping position.
- Note whether the pain is located at the top of the shoulder, inside the joint, or in the upper trapezius region between the neck and shoulder tip.
- Note whether the pain is improving, static, or progressively worsening over weeks, as this progression pattern guides the urgency of evaluation.
Risk Factors That Increase Shoulder Pain Likelihood in Women
Several named risk factors increase the probability that a woman will develop shoulder pain, and understanding which apply to a specific individual helps guide the prioritization of diagnostic evaluation.
Age is one of the strongest predictors. Rotator cuff degeneration is nearly universal after age 60 on imaging, even in asymptomatic shoulders. Frozen shoulder has a well-established peak incidence between 40 and 60 years in women. Polymyalgia rheumatica rarely presents before age 60.
Diabetes mellitus, regardless of type, increases frozen shoulder risk three to five times. The mechanism involves advanced glycation end-products stiffening glenohumeral joint capsule collagen. Women with type 2 diabetes or PCOS-related insulin resistance face this risk and should report early shoulder stiffness to their primary care physician rather than waiting for significant functional limitation.
| Risk Factor | Shoulder Condition Increased | Mechanism | Degree of Risk Increase |
|---|---|---|---|
| Postmenopause (no HRT) | Rotator cuff degeneration, frozen shoulder | Estrogen withdrawal, reduced collagen synthesis | Moderate to high |
| Diabetes mellitus | Frozen shoulder (adhesive capsulitis) | AGE-collagen cross-linking in joint capsule | 3-5x increased risk |
| Hypothyroidism | Adhesive capsulitis, tendon stiffness | Myxedematous capsular deposits, reduced collagen turnover | Moderate |
| Rheumatoid arthritis | Shoulder synovitis, joint destruction | TNF-alpha, IL-6 mediated synovial inflammation | High |
| Lupus (SLE) | Shoulder arthritis, avascular necrosis | Immune complex deposition, corticosteroid side effects | High |
| Overhead occupational exposure | Rotator cuff tendinopathy, bursitis | Mechanical subacromial impingement | Cumulative, dose-dependent |
| Sedentary desk work | Subacromial impingement, trapezius strain | Scapular dyskinesis, muscle fatigue | Moderate |
| Pregnancy | Glenohumeral laxity, postural strain | Relaxin-mediated ligament laxity, postural compensation | Low to moderate |
| Prior shoulder injury | Recurrent instability, early OA | Capsular laxity, cartilage damage | Moderate to high |
| Family history of autoimmune disease | RA, SLE, polymyalgia rheumatica | Genetic immune dysregulation | Moderate |
Prior shoulder injury is an independent risk factor. Women with a history of glenohumeral dislocation, labral tear, or significant rotator cuff injury face accelerated degenerative changes at the shoulder joint regardless of age, because cartilage damage from prior injury changes the loading pattern of the entire joint complex.
Key Takeaway: Diabetes, hypothyroidism, postmenopausal status, and a prior shoulder injury are among the most actionable risk factors for shoulder pain in women, and each has a specific named biological mechanism that a provider can assess and sometimes address directly.
How Doctors Diagnose the Cause of Shoulder Pain in Women
Diagnosing the specific cause of shoulder pain in a woman requires a structured approach that accounts for her hormonal status, medical history, occupational exposures, and the specific characteristics of the pain itself, not simply a physical examination of the shoulder in isolation.
A thorough clinical history is the starting point. The provider will typically ask about the onset and duration of pain, which movements or positions aggravate or relieve it, whether there is associated stiffness (particularly in the morning), whether the pain is unilateral or bilateral, whether there are systemic symptoms (fever, rash, fatigue, weight loss), and whether there is any relationship to menstrual cycle phase, pregnancy, or menopause. This history alone narrows the differential significantly.
Physical examination of the shoulder includes a series of named provocative tests:
- Neer impingement test: pain produced by passive internal rotation of the arm while elevated suggests subacromial impingement
- Hawkins-Kennedy test: pain produced by internal rotation at 90 degrees of flexion suggests rotator cuff impingement
- Drop arm test: inability to slowly lower the arm from 90 degrees of abduction suggests a significant rotator cuff tear
- Empty can test: pain or weakness during resisted abduction with the arm in internal rotation isolates the supraspinatus tendon
- Cross-body adduction test: pain at the top of the shoulder during this movement suggests AC joint pathology
- Range of motion assessment: all four cardinal directions (elevation, external rotation, internal rotation, abduction) are assessed; global restriction in all directions suggests adhesive capsulitis
Imaging follows the history and examination. A plain X-ray (radiograph) evaluates bony structures: the acromion shape, clavicle position, glenohumeral joint space, and any calcification within the supraspinatus tendon. Magnetic resonance imaging (MRI) provides detailed soft tissue evaluation of the rotator cuff tendons, labrum, joint capsule, and bursa. Musculoskeletal ultrasound allows dynamic assessment of tendon integrity and bursal fluid volume.
Blood tests are ordered when autoimmune or systemic causes are suspected. These include C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), anti-CCP antibodies, rheumatoid factor (RF), antinuclear antibody (ANA), and thyroid-stimulating hormone (TSH) with free T4. Women presenting with bilateral shoulder involvement, morning stiffness exceeding 45 minutes, or systemic symptoms should have this inflammatory and autoimmune panel ordered early rather than after failed mechanical treatment.
When Shoulder Pain in Women Requires Urgent or Emergency Care
Most shoulder pain in women is not an emergency. But a defined set of presentations require immediate evaluation and should not be monitored at home, treated with over-the-counter pain medication, or scheduled for a next-available appointment.
A woman should see her primary care physician within 48 hours, not waiting weeks, if her shoulder pain:
- Has persisted for more than 2 weeks without an obvious mechanical cause or improvement
- Is accompanied by fever or chills (raises concern for septic arthritis, which can destroy a joint in 24 to 48 hours if untreated)
- Is associated with marked bilateral stiffness upon waking, lasting more than an hour
- Involves progressive loss of shoulder range of motion over weeks
- Is in a woman who has diabetes, thyroid disease, or an autoimmune condition
She should contact a board-certified orthopedic surgeon for evaluation within one to two weeks if:
- There is a history of trauma followed by persistent weakness of the arm
- She cannot lift her arm above shoulder height due to weakness rather than pain
- She has a known rotator cuff condition that has worsened despite conservative management
Emergency Symptoms: When to Call 911 or Go to the ER
Certain presentations associated with shoulder pain in women require immediate emergency evaluation. Do not wait to see if these resolve on their own.
Call 911 or go to the nearest emergency room immediately if you experience:
- Left shoulder pain accompanied by chest pressure, tightness, or heaviness (possible myocardial infarction: the AHA confirms women frequently present without classic chest pain)
- Left shoulder pain with shortness of breath, nausea, sweating, or unusual fatigue at rest
- Left shoulder or jaw pain that develops suddenly during exertion or emotional stress
- Right shoulder pain accompanied by sudden severe upper right abdominal pain, jaundice (yellowing of skin or eyes), or fever (possible acute cholecystitis or biliary emergency)
- Shoulder pain following any trauma with visible joint deformity, inability to move the arm at all, or numbness of the entire hand or arm (possible dislocation, fracture, or brachial plexus injury)
- Shoulder pain with severe headache, one-sided weakness, facial drooping, or difficulty speaking (possible stroke with atypical shoulder referral)
- Right shoulder pain accompanied by severe lower abdominal pain, vaginal bleeding, and a known or possible pregnancy (possible ectopic pregnancy rupture with phrenic nerve-referred shoulder pain)
These presentations can indicate myocardial infarction, biliary emergency, obstetric emergency, or acute neurovascular injury, and they require emergency medical assessment, not an urgent care appointment or a phone call.
Frequently Asked Questions About Causes of Shoulder Pain in Females
What is the most common cause of shoulder pain in women?
Rotator cuff tendinopathy and adhesive capsulitis (frozen shoulder) are the two most common structural causes of shoulder pain in women, with frozen shoulder affecting women at approximately twice the rate it affects men.
Rotator cuff problems typically produce pain with overhead arm movement, while frozen shoulder produces progressively worsening stiffness and restricted range of motion in all directions.
A primary care physician or board-certified orthopedic surgeon can differentiate these based on physical examination and, when needed, MRI of the shoulder.
Can hormones cause shoulder pain in females?
Yes, female hormones directly influence shoulder joint health through named biological pathways.
Estrogen supports tendon collagen synthesis and suppresses pro-inflammatory cytokines; when estrogen declines at perimenopause and menopause, these protective effects diminish, accelerating tendon degeneration and increasing frozen shoulder susceptibility.
Thyroid hormone imbalance, particularly hypothyroidism, which is seven times more common in women than men, produces capsular stiffening that can mimic or trigger frozen shoulder.
Why does my left shoulder hurt as a woman?
Left shoulder pain in women most commonly originates from the rotator cuff, acromioclavicular joint, or periscapular muscles on the left side due to postural, occupational, or mechanical causes.
However, the American Heart Association specifically identifies left shoulder pain as one of the atypical symptoms of myocardial infarction more commonly reported by women than by men.
If left shoulder pain occurs alongside chest discomfort, shortness of breath, nausea, sweating, or jaw pain, call 911 immediately rather than treating it as a musculoskeletal complaint.
What does shoulder pain from a heart attack feel like in a woman?
Women experiencing a heart attack often describe left shoulder pain as an aching, heaviness, or pressure rather than a sharp or stabbing sensation.
This referred pain reaches the shoulder through the phrenic nerve pathway, which shares dermatomal territory with the left shoulder at cervical levels C3, C4, and C5, and is produced by diaphragmatic irritation from ischemia of the inferior myocardial wall.
The AHA reports that women are more likely than men to experience this atypical presentation and less likely to have the classic central crushing chest pain, which increases the risk of delayed diagnosis.
When should a woman see a doctor for shoulder pain?
A woman should contact her primary care physician if shoulder pain persists longer than two weeks, is accompanied by fever, involves progressive loss of motion, or occurs in the context of diabetes, thyroid disease, or an autoimmune condition.
She should seek same-day emergency evaluation if pain is accompanied by chest pressure, shortness of breath, nausea, or jaw pain on the left side, or if right shoulder pain accompanies severe abdominal pain or pregnancy.
Any shoulder pain that follows significant trauma and involves an inability to lift the arm warrants emergency room evaluation to rule out fracture, dislocation, or nerve injury.
Can pregnancy cause shoulder pain?
Yes, pregnancy causes shoulder pain through multiple mechanisms including relaxin-mediated glenohumeral joint laxity, postural compensation for the shifting center of gravity, and, in late pregnancy, referred diaphragmatic pain from conditions like HELLP syndrome.
The American College of Obstetricians and Gynecologists recognizes relaxin as a systemically acting hormone that reduces connective tissue stiffness throughout the body, not only in the pelvis, which can worsen pre-existing shoulder instability.
Right shoulder pain during pregnancy accompanied by upper abdominal pain, elevated blood pressure, or swelling is a potential obstetric emergency requiring immediate evaluation at a hospital labor and delivery unit.
Closing
Shoulder pain in women is not a single condition. It is a clinical signal that can originate from the rotator cuff, the joint capsule, the acromioclavicular joint, the bursa, the immune system, the thyroid, the gallbladder, or the heart, and which source is driving the pain matters enormously for what happens next.
The biological reason women face a higher burden from certain shoulder conditions is not coincidence. Estrogen’s role in tendon and joint capsule health, relaxin’s effect during pregnancy, thyroid hormones’ influence on connective tissue, and the immune system’s sex-biased activation are all specific, named mechanisms with real clinical consequences. Understanding those mechanisms helps a woman recognize why her shoulder pain may be tied to her hormonal status or reproductive stage rather than a workout injury.
If your shoulder pain has lasted more than two weeks, is worsening rather than improving, or comes with any systemic symptoms like fever, morning stiffness, or the cardiac warning signs described above, bring this article’s specifics to your primary care physician or board-certified orthopedic surgeon. You now know the right questions to ask and the right clinical context to provide. That puts you ahead of where most patients start.