Rotator Cuff Tear Symptoms: Full 2026 Clinical Guide
Rotator cuff tear symptoms typically include deep shoulder pain, arm weakness, restricted motion, and sleep-disrupting night pain, and the exact pattern of symptoms depends on which tendon is torn, how severely, and whether the tear happened suddenly or developed over months or years. Understanding these symptoms precisely, not just knowing “shoulder pain exists,” is what helps you recognize where your situation falls on the clinical severity spectrum.
According to the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), rotator cuff injuries are among the most common causes of shoulder pain in adults, affecting millions of Americans each year, with full-thickness tears occurring in roughly 20 to 30 percent of people over age 60. That number rises to nearly 80 percent in autopsy studies of individuals over age 80, much of it clinically silent, which means the presence of a tear on imaging does not automatically determine whether symptoms exist or how severe they are.
This guide covers every recognized symptom of a rotator cuff tear with the specific physiological mechanism behind each one, explains how symptoms differ between partial and full-thickness tears, identifies who is most at risk for atypical presentations, and gives you the clinical framework to know when a scheduled appointment is appropriate versus when your situation calls for same-day evaluation.
Rotator Cuff Tear Symptoms: What This Injury Actually Feels Like
Rotator cuff tear symptoms feel like a persistent, deep shoulder ache that worsens with specific movements, particularly lifting the arm overhead, reaching behind the back, or lying on the affected side, and in more severe tears, like a sudden loss of strength that makes the arm feel heavy or unresponsive.
The experience is distinct from superficial muscle soreness. The pain originates from inside the shoulder joint and from the subacromial space, the narrow corridor between the top of the humerus (upper arm bone) and the undersurface of the acromion (the bony projection of the scapula). When the supraspinatus tendon tears, even partially, it triggers an inflammatory response in the adjacent subacromial bursa, a fluid-filled sac that normally reduces friction. That bursal inflammation, driven by prostaglandin E2 and interleukin-1 beta, generates the characteristic deep aching quality that most patients describe.
The pain location is usually the top and outer side of the shoulder, sometimes radiating into the outer upper arm but rarely below the elbow. Pain that travels into the forearm, hand, or fingers suggests nerve involvement rather than an isolated rotator cuff problem.
Key physical sensations people report with rotator cuff tears:
- A dull, deep ache in the shoulder that does not go away with rest in more advanced cases
- Sharp, catching pain at a specific point in arm elevation, typically between 60 and 120 degrees (the painful arc)
- Weakness when trying to lift objects or raise the arm to shoulder height
- A sense of instability or giving way in the shoulder during overhead tasks
- Pain when reaching across the body or tucking a shirt in at the back
People with diabetes mellitus may experience a rotator cuff tear that is complicated by adhesive capsulitis (frozen shoulder), which adds severe global motion restriction to the typical symptom pattern. Their presentation can look more like frozen shoulder than a classic tear, which delays accurate diagnosis.
Symptoms of a Torn Rotator Cuff: The Full Clinical Picture
The full clinical picture of a torn rotator cuff includes shoulder pain, directional arm weakness, motion restriction, night pain, and in some cases audible or palpable shoulder crepitus, with the specific combination of symptoms pointing clearly to which tendon or tendons are involved.
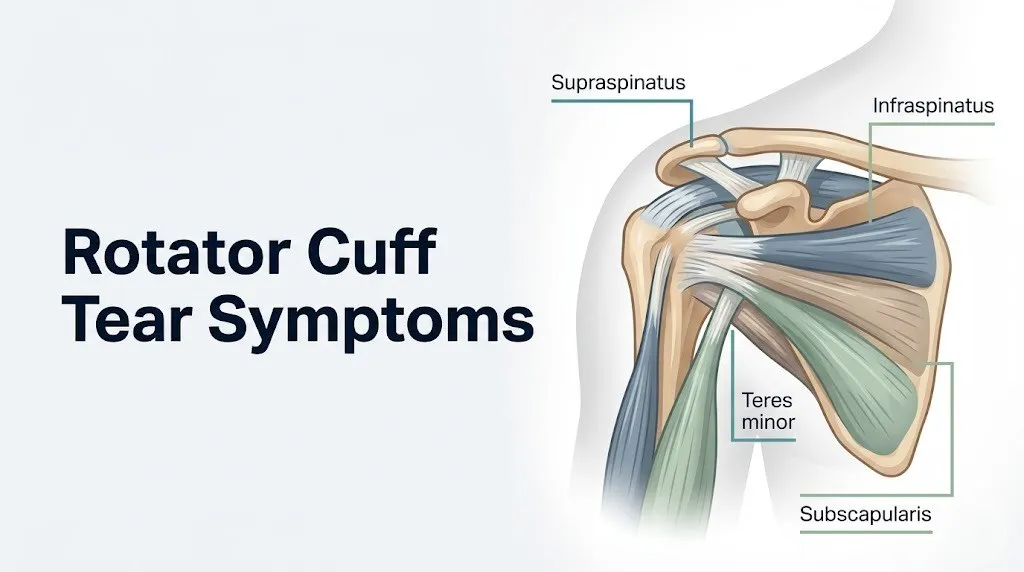
Each of the four rotator cuff tendons produces a distinct weakness pattern when torn. This is not a detail buried in orthopedic textbooks. It is a practically useful clinical fact. Knowing that your weakness is in arm elevation versus external rotation versus internal rotation helps a clinician identify which tendon is involved before imaging is even ordered.
| Tendon | Primary Function | Symptom When Torn | Clinical Test |
|---|---|---|---|
| Supraspinatus | Initiates arm abduction (0 to 30 degrees), depresses humeral head | Weakness lifting arm away from side, pain at 90-degree elevation | Jobe empty can test |
| Infraspinatus | External rotation of the arm | Weakness rotating arm outward, difficulty reaching behind | External rotation lag sign |
| Teres minor | Assists external rotation, inferior humeral head stabilization | External rotation weakness (combined with infraspinatus), posterior shoulder pain | Hornblower’s sign |
| Subscapularis | Internal rotation, anterior joint stabilization | Weakness pushing arm inward and forward, difficulty reaching behind back | Lift-off test, belly press test |
Most degenerative rotator cuff tears begin in the supraspinatus tendon, specifically at the avascular “critical zone” 1 cm proximal to its insertion on the greater tuberosity of the humerus. This zone has the poorest blood supply, making it the weakest point mechanically.
The full clinical picture in a large or massive tear can also include visible or palpable muscle atrophy above the scapular spine (supraspinatus atrophy) or below it (infraspinatus atrophy), which becomes apparent when the shoulder is inspected from behind. Muscle bulk loss in these locations indicates chronic tendon disconnection with progressive denervation-like atrophy.
Older adults, particularly those over 70, may present with a rotator cuff tear that has been silently enlarging for years before the first clinical symptom appears. Their first complaint is often not acute pain but rather a gradual inability to reach overhead for household tasks.
What Is a Rotator Cuff Tear and Why Does It Cause Symptoms
A rotator cuff tear is a disruption of one or more of the four tendons that form the rotator cuff, the musculotendinous sleeve surrounding the glenohumeral joint, and it causes symptoms because it disrupts the dynamic force-couple mechanism that keeps the humeral head centered in the glenoid socket during arm movement.
Think of the glenohumeral joint like a golf ball balanced on a tee. The ball (humeral head) sits on the tee (glenoid fossa), which is shallow and provides almost no inherent bony stability. The rotator cuff is the muscular system that constantly adjusts and compresses the ball onto the tee during movement. When a tear disrupts that compression mechanism, the ball starts to slide, creating abnormal forces, pinching soft tissue structures, and triggering inflammation.
The glenohumeral joint is a ball-and-socket synovial joint with the greatest range of motion of any joint in the human body, which also makes it the most mechanically dependent on soft tissue support. The price of that mobility is vulnerability. Tendons working through an enormous range of motion under heavy loads, repetitively, across decades, are prone to mechanical fatigue at their least-vascularized zones.
Two distinct tear mechanisms operate differently. Traumatic tears result from acute force applied to the shoulder, such as a fall on an outstretched arm or a sudden violent pull. Degenerative tears result from cumulative micro-damage exceeding the tendon’s repair capacity over years. A 2019 analysis published in the Journal of Bone and Joint Surgery found that degenerative tears account for the majority of rotator cuff tears in individuals over 50, while traumatic tears are more common in younger adults following contact sports or occupational injuries.
Key Takeaway: A rotator cuff tear causes symptoms by disrupting the force-couple that keeps the humeral head centered in its socket, triggering bursal inflammation via prostaglandin E2, and producing a distinct weakness pattern depending on which of the four tendons is torn.
Shoulder Pain: The Primary Symptom of a Rotator Cuff Tear
Shoulder pain is the primary and most consistent symptom of a rotator cuff tear, typically described as a deep ache on the top or outer side of the shoulder that worsens with overhead activity, reaching, and lying on the affected side.
The pain mechanism is two-pronged. First, mechanical: when torn tendon fibers cannot properly compress the humeral head, arm movement causes abnormal tissue impingement in the subacromial space. Second, inflammatory: the injured tendon and the secondarily inflamed subacromial bursa release prostaglandin E2, which sensitizes nociceptors (pain-sensing nerve endings) in the surrounding tissue. These nociceptors are innervated by branches of the suprascapular nerve and the axillary nerve, both arising from the brachial plexus (C5-C6 nerve roots).
The painful arc phenomenon is a classic clinical sign. Pain increases as the arm is elevated from roughly 60 to 120 degrees of abduction and then decreases above 120 degrees. This arc corresponds to the angular range at which the supraspinatus tendon and subacromial bursa are most compressed against the undersurface of the acromion. Below 60 degrees and above 120 degrees, the compression temporarily resolves, which is why the pain has this characteristic mid-range spike.
Pain referral patterns in rotator cuff tears can mislead both patients and clinicians:
- Outer upper arm ache is common and follows the territory of the axillary nerve
- Pain at the lateral neck is occasionally reported and represents referred pain from the brachial plexus level
- Pain below the elbow is not typical of an isolated rotator cuff tear and should prompt evaluation for cervical radiculopathy or concurrent biceps tendon pathology
Women in the perimenopause or postmenopause phase may notice that shoulder pain is more persistent than they expect from a minor injury. Research published in the American Journal of Sports Medicine has identified estrogen’s role in maintaining type I collagen integrity in tendons. As estrogen levels decline after menopause, tendon tensile strength decreases, making the rotator cuff more susceptible to both injury and prolonged pain following injury.
Arm Weakness and a Rotator Cuff Tear: Why Strength Disappears
Arm weakness in a rotator cuff tear occurs because the torn tendon can no longer generate its full contribution to the muscular force couple of the glenohumeral joint, producing directional strength deficits that correspond precisely to the function of the affected tendon.
Weakness is not the same as pain inhibition. Two distinct types of shoulder weakness exist in rotator cuff pathology. Pain-inhibited weakness occurs when the arm could generate normal force mechanically, but pain causes the patient to reflexively limit effort. True tendon-disconnection weakness occurs when the tendon has torn completely or significantly enough that the muscle cannot transmit its force to the humeral head regardless of effort. Clinical tests like the drop arm test distinguish between these two categories.
The drop arm test is one of the most instructive clinical signs. The examiner elevates the patient’s arm to 90 degrees of abduction and releases it. In a complete supraspinatus tear, the patient cannot sustain that position and the arm drops suddenly to the side. A 2017 systematic review in the Journal of Shoulder and Elbow Surgery found the drop arm test has a specificity of approximately 97 percent for full-thickness supraspinatus tears, making it highly reliable when positive.
Weakness patterns by tendon:
- Supraspinatus tear: weakness in the first 30 degrees of arm elevation from the side (abduction), difficulty lifting objects away from the body at waist or hip height
- Infraspinatus or teres minor tear: weakness in external rotation, difficulty turning a door handle or throwing a ball, often noticed as a “dead arm” feeling
- Subscapularis tear: weakness in internal rotation, difficulty pushing a revolving door, trouble reaching behind the back to fasten clothing
Individuals who have used the affected arm through a period of progressive tendon damage may have developed compensatory movement patterns. They may use the deltoid muscle excessively to initiate arm elevation, which can delay recognition of supraspinatus weakness until functional testing isolates the specific motion.
Limited Range of Motion in a Rotator Cuff Tear
Limited range of motion in a rotator cuff tear reflects both pain-protective restriction, where the brain limits motion to avoid provoking pain, and mechanical restriction, where scar tissue, tendon retraction, or muscle contracture physically prevent full motion.
Early and partial rotator cuff tears typically preserve most range of motion. The patient can still reach overhead but finds specific positions painful or weak. Advanced tears, particularly those that have been present for months or years without treatment, can develop secondary adhesive capsulitis as the glenohumeral joint capsule thickens and contracts in response to chronic disuse and inflammation.
The distinction between motion limited by pain (which improves when the pain stimulus is removed) and motion limited by capsular contracture (which does not improve with pain removal) is clinically important. Assessing passive range of motion, where the examiner moves the arm rather than the patient, separates these two causes. When passive motion is also limited, capsular involvement is likely.
Specific motion restrictions in rotator cuff tears by pattern:
| Motion | Normal Range | Common Restriction with Tear | Clinical Implication |
|---|---|---|---|
| Forward flexion (reaching overhead) | 0 to 180 degrees | 120 to 150 degrees in moderate tears | Supraspinatus and deltoid involvement |
| Abduction (arm out to the side) | 0 to 180 degrees | 90 to 120 degrees | Supraspinatus primary limitation |
| External rotation | 60 to 90 degrees | 30 to 50 degrees in large tears | Infraspinatus and capsular involvement |
| Internal rotation (hand behind back) | Reach to T7 level | Reduced to gluteal level | Subscapularis and capsular involvement |
People with rheumatoid arthritis affecting the shoulder may have motion restriction from joint synovitis superimposed on rotator cuff pathology. Their motion loss may be more global and more painful than expected from the cuff tear alone, requiring evaluation by both a board-certified orthopedic surgeon and a rheumatologist to address both pathologies simultaneously.
Key Takeaway: Arm weakness in a rotator cuff tear follows a specific directional pattern determined by which tendon is torn, with supraspinatus tears causing abduction weakness, infraspinatus tears causing external rotation weakness, and subscapularis tears causing internal rotation weakness.
Night Pain and a Rotator Cuff Tear: Why Sleep Gets Disrupted
Night pain is one of the most diagnostically telling symptoms of a rotator cuff tear, occurring in up to 70 percent of patients with full-thickness tears, and its mechanism is directly related to sleeping position and the anatomy of the subacromial space.
When a person lies on the affected shoulder (lateral recumbent position), body weight compresses the outer shoulder against the mattress. This pressure transmits directly through the deltoid and into the subacromial space, narrowing it and pressing the inflamed subacromial bursa and injured tendon against the undersurface of the acromion. The result is a sharp, awakening pain at the outer shoulder that forces the person to shift position.
Even sleeping on the opposite shoulder causes problems for many patients. In that position, the affected arm hangs forward across the body, placing the supraspinatus tendon in a position of internal rotation that stretches and stresses the already-inflamed tissue. Many patients eventually resort to sleeping in a recliner or a semi-upright position, which reduces dependent arm traction.
To improve sleep positioning with a suspected rotator cuff tear:
- Avoid lying directly on the affected shoulder. Use a firm pillow to support the arm in a neutral position.
- When lying on the opposite side, place a pillow between the chest and the affected arm to prevent it from crossing the body midline.
- A semi-reclined sleeping position (30 to 45 degrees) reduces gravitational tension on the supraspinatus tendon and often dramatically reduces night pain.
- Avoid sleeping with the arm raised above the head, which maximally narrows the subacromial space.
- Report the specific sleep position that triggers pain to your clinician. This information helps localize which structure is most irritable.
Night pain that does not respond to positioning changes, persists even in a recliner, or is accompanied by fever, sweating, or unexplained weight loss should be evaluated promptly. These accompanying symptoms can indicate shoulder septic arthritis or, in rare cases, a shoulder tumor, neither of which should be monitored at home.
Clicking and Popping Sounds With a Rotator Cuff Tear
Audible clicking or popping sounds (crepitus) with shoulder movement occur in some rotator cuff tears, produced when roughened or irregular tendon tissue catches on adjacent structures during the arc of motion.
Not all shoulder clicking indicates pathology. Benign shoulder clicking without pain is common and represents normal fluid dynamics or minor joint surface irregularities. The clinically relevant crepitus in rotator cuff disease has three defining characteristics: it is accompanied by pain, it occurs at a consistent point in the range of motion, and it is reproducible on repeated testing.
The mechanism behind rotator cuff-related crepitus involves the torn or frayed tendon edge catching on the anterior edge of the acromion or the coracoacromial ligament as the arm moves through the subacromial space. Think of a frayed rope running through a tight pulley. Each cycle produces a catching sensation or audible snap when the frayed fibers pass through the narrowed space.
Types of shoulder sounds in rotator cuff disease:
- Soft clicking during rotation: often represents minor tendon irregularity or bicipital groove friction, usually benign
- A palpable “clunk” with arm elevation: suggests a larger tendon flap catching under the coracoacromial arch, more likely to be clinically significant
- Grinding or grating crepitus throughout motion: suggests glenohumeral joint surface involvement (osteoarthritis or chondral damage), which may coexist with a rotator cuff tear in older adults
- A single sharp pop at the moment of injury: suggests acute tendon rupture, a presentation requiring urgent evaluation
According to the American Academy of Orthopaedic Surgeons, shoulder crepitus that is consistently painful and reproducible warrants imaging to assess the integrity of the rotator cuff tendons and the glenohumeral joint surfaces. Crepitus alone, without pain or functional limitation, rarely requires intervention.
Symptoms of a Partial Versus Full-Thickness Rotator Cuff Tear
The symptoms of a partial-thickness rotator cuff tear and a full-thickness rotator cuff tear differ primarily in the degree of functional loss, with partial tears typically causing pain and mild weakness while full-thickness tears produce more substantial strength deficits and, in massive tears, an inability to elevate the arm at all.
A partial-thickness tear does not extend completely through the tendon. Fibers on one surface (either the articular surface facing the joint or the bursal surface facing the subacromial bursa) are disrupted, but continuity of the tendon is partially preserved. A full-thickness tear extends entirely from the articular to the bursal surface, creating a complete hole in the tendon that the muscle can no longer bridge.
| Feature | Partial-Thickness Tear | Full-Thickness Tear | Massive Tear (Greater than 5 cm) |
|---|---|---|---|
| Pain level | Moderate, activity-dependent | Moderate to severe | Severe, often constant |
| Arm elevation | Usually preserved | May be preserved with compensation | Often impossible |
| Strength deficit | Mild, task-specific | Moderate, directional | Marked, global |
| Night pain | Common | Common and severe | Severe, multiple positions |
| Functional impact | Difficulty with overhead tasks | Difficulty with daily activities | Significant disability |
| Spontaneous healing potential | Possible with physical therapy | Limited without surgery | Unlikely without surgical repair |
A partial tear can progress to a full-thickness tear over time, particularly without treatment or with continued provocative activity. A 2021 study published in the Journal of Shoulder and Elbow Surgery found that untreated partial-thickness supraspinatus tears progressed to full-thickness tears in approximately 40 percent of cases followed over five years, with progression rate correlating with initial tear size and patient age.
Younger patients (under 50) with partial tears generally respond better to conservative management. Patients over 65 with newly identified full-thickness tears have a narrower window for surgical repair because fatty infiltration of the rotator cuff muscles begins within weeks of complete tendon disconnection and progresses over months, reducing the feasibility and outcome quality of surgical repair.
Key Takeaway: Partial rotator cuff tears typically allow continued arm elevation with mild weakness, while full-thickness tears produce more substantial functional loss, and untreated partial tears progress to full-thickness in roughly 40 percent of cases within five years.
Early Symptoms of a Rotator Cuff Tear: What Comes First
Early rotator cuff tear symptoms often begin as a dull ache in the outer shoulder that appears specifically during or after overhead activity, a symptom pattern so mild and intermittent that most people attribute it to muscle fatigue or a minor strain.
Degenerative tears, the most common type, typically announce themselves subtly. The supraspinatus tendon has been accumulating micro-damage for years in its avascular critical zone. The first clinical symptom usually appears when accumulated damage reaches the threshold where the remaining intact fibers can no longer handle normal loads without provoking inflammation. At that point, the shoulder aches after throwing a ball, painting a ceiling, or lifting a bag into an overhead bin. The ache resolves with rest. This pattern repeats for weeks or months before the person connects the dots.
Early warning signs that distinguish a beginning rotator cuff problem from ordinary muscle soreness:
- Pain that is specifically worse with overhead activity and not with activities that keep the arm below shoulder height
- Ache that begins during activity and lingers for one to two hours afterward, rather than resolving immediately with rest
- Weakness that appears only at the end range of arm elevation, rather than being present throughout all arm movements
- Discomfort that localizes to the outer shoulder or upper arm rather than the muscle belly of the deltoid
- Sleep disruption on the first night after heavy shoulder use, even without daytime symptoms
According to MedlinePlus, published by the U.S. National Library of Medicine, many rotator cuff injuries begin with gradual onset of pain and limited strength, and delaying evaluation allows the tear to expand and associated muscle to atrophy, both of which complicate eventual treatment.
Early presentation in athletes tends to be more specific. A baseball pitcher may notice a velocity drop or loss of command before pain becomes prominent. A swimmer may feel fatigue in the shoulder stroke at a point in training that previously felt comfortable. These performance-based early signals are often the first clinical indicator in high-demand athletes.
Symptoms of a Bad Rotator Cuff: Advanced and Progressive Signs
A severely damaged or “bad” rotator cuff, clinical language for a large or massive full-thickness tear, produces symptoms that have moved well beyond pain into functional disability, including visible muscle wasting, profound strength loss, and in some cases a structural inability to raise the arm against gravity.
The term “bad rotator cuff” colloquially describes what clinicians classify as a massive rotator cuff tear, defined as a tear extending at least 5 cm or involving two or more tendons completely. At this stage, the force-couple mechanism of the glenohumeral joint is so severely disrupted that the deltoid muscle cannot compensate. The humeral head migrates superiorly and contacts the undersurface of the acromion directly, producing a condition called cuff tear arthropathy in advanced cases.
Observable signs of an advanced rotator cuff tear:
- Visible hollowing or wasting above and below the scapular spine (supraspinatus and infraspinatus atrophy)
- Complete inability to initiate arm elevation from the side without compensatory trunk lean or shrugging
- Pseudoparalysis: the arm hangs at the side and the patient cannot raise it above 90 degrees despite no neurological deficit
- Severe constant pain that does not fully resolve with rest, heat, or over-the-counter analgesics
- Palpable or visible shoulder deformity from chronic superior humeral head migration
- Audible or palpable grinding (glenohumeral crepitus) during any shoulder movement, suggesting cartilage involvement
Cuff tear arthropathy is an end-stage complication described by the American Academy of Orthopaedic Surgeons in which chronic full-thickness tear leads to superior humeral head migration, acromial erosion, and eventual glenohumeral arthrosis. Standard rotator cuff repair surgery cannot address this stage. Patients with cuff tear arthropathy require evaluation for reverse total shoulder arthroplasty, a procedure specifically designed for this presentation.
Men over 65 who have worked in physically demanding occupations (construction, overhead manufacturing, farming) are disproportionately represented in massive tear populations. Their occupation-related cumulative tendon loading, combined with age-related avascular zone degeneration, creates a compounding risk that often results in bilateral large tears by their 60s.
Rotator Cuff Tear Symptoms in Older Adults
Rotator cuff tear symptoms in older adults are often more severe at diagnosis than in younger patients, because age-related changes in tendon vascularity, collagen quality, and healing capacity allow tears to enlarge silently over months or years before functional loss forces a clinical visit.
The aging supraspinatus tendon has two distinct vulnerabilities that younger tendons do not share. First, the avascular critical zone becomes even more poorly perfused after age 60, accelerating degenerative fiber failure. Second, age-related decline in type I collagen synthesis (driven partly by declining testosterone in men and estrogen in women) reduces the tendon’s tensile strength and its capacity for intrinsic repair.
According to the NIAMS, the prevalence of full-thickness rotator cuff tears rises from approximately 13 percent in adults in their 50s to more than 50 percent in adults over 80, though a substantial proportion of these tears are asymptomatic. The presence of a tear on imaging does not automatically explain a patient’s pain; the clinical examination must correlate the imaging finding with the functional presentation.
Specific considerations for older adults with rotator cuff symptoms:
- Weakness may be misattributed to sarcopenia (age-related muscle loss) rather than tendon pathology
- Bilateral rotator cuff involvement is more common in older adults; the non-dominant shoulder may be symptomatic but overlooked
- Concurrent glenohumeral osteoarthritis complicates the symptom picture, adding joint-line tenderness and end-range grinding to the typical cuff tear presentation
- Post-surgical healing in older adults is slower and may be incomplete if surgery is delayed until massive fatty infiltration of the cuff muscles has occurred; a board-certified orthopedic surgeon should assess surgical candidacy early when a large tear is identified in a functionally active older adult
Older adults who take long-term systemic corticosteroids (for conditions like rheumatoid arthritis, COPD, or polymyalgia rheumatica) face an additional risk: corticosteroids impair type I collagen synthesis, accelerate tendon degeneration, and can cause spontaneous tendon rupture at lower force thresholds than expected.
Key Takeaway: Rotator cuff tear symptoms in adults over 60 are frequently more severe than expected at diagnosis because age-related tendon degeneration allows tears to grow silently, and concurrent osteoarthritis can mask the specific weakness patterns that signal tendon involvement.
Rotator Cuff Tear Symptoms in Athletes and Active Individuals
Athletes and active individuals with rotator cuff tears often present differently from sedentary adults, because athletic conditioning can partially compensate for tendon deficits, masking the strength loss and range of motion changes that would otherwise be clinically obvious.
Overhead athletes, including baseball pitchers, swimmers, volleyball players, and tennis players, subject the rotator cuff to extraordinarily high repetitive loads. A professional baseball pitcher places the supraspinatus, infraspinatus, and subscapularis under forces exceeding six times the weight of the arm during deceleration after ball release. This load pattern creates a specific injury pattern: posterior-superior partial-thickness articular-side tears at the infraspinatus and supraspinatus insertion, a pattern distinct from the anterior bursal-side tears more common in degenerative disease.
Symptom presentation in overhead athletes:
- Pain specifically during the late cocking or acceleration phase of throwing, not at rest
- A drop in throwing velocity or racket speed without obvious pain, representing pain-inhibited muscular output
- “Dead arm” sensation: the arm feels heavy and disconnected immediately after high-effort activity
- Loss of command or accuracy in throwing athletes before pain intensity becomes disabling
- Recovery time after workouts increasing progressively over a season
Quick Tip:
- An athlete who notices velocity drop or technique changes before shoulder pain should consider a rotator cuff evaluation rather than attributing the change to fatigue alone
- Physical conditioning in overhead athletes can preserve functional arm elevation even with a partial tear, delaying diagnosis by months
- Female overhead athletes, particularly swimmers and volleyball players, may have a higher risk of rotator cuff pathology during high-training-volume phases of their cycle when estrogen fluctuations temporarily reduce tendon stiffness
A sports medicine physician or a board-certified orthopedic surgeon with experience in sports shoulder pathology should evaluate an athlete with progressive shoulder symptoms that affect performance, particularly if shoulder pain has been present for more than three to four weeks without improvement despite activity modification.
Symptoms of a Rotator Cuff Tear Requiring Urgent Evaluation
Certain presentations of rotator cuff tear symptoms require evaluation within 24 to 72 hours rather than a routine appointment scheduled weeks away, because delayed assessment in these circumstances can allow the condition to worsen in ways that reduce treatment options.
The clinical distinction between “watch and wait with activity modification” and “this needs to be evaluated now” is something the top five Google results for this keyword fail to address with precision. A general “see a doctor” sentence does not help a person determine whether they need an urgent care visit tomorrow or an emergency room visit tonight.
Symptoms that warrant evaluation within 24 to 72 hours:
- Sudden complete loss of shoulder strength following a fall, direct impact, or forced arm movement, particularly if accompanied by immediate severe pain
- Inability to lift the arm above waist height at all after an acute injury
- Rapid onset of visible swelling or bruising around the shoulder girdle after trauma
- Numbness or tingling down the arm following a shoulder injury (suggests possible brachial plexus involvement)
- Any rotator cuff symptom in a patient with known rheumatoid arthritis that dramatically worsens over 24 to 48 hours, as inflammatory flare can cause rapid tendon destruction
Symptoms appropriate for a scheduled appointment within one to two weeks:
- Shoulder ache that has been gradually worsening over several weeks without a specific injury event
- Night pain that has appeared or worsened over the past two to four weeks
- Progressive weakness in specific arm directions noticed during normal daily tasks
- Audible clicking accompanied by pain at a consistent point in the range of motion
Contact a primary care physician or a sports medicine physician within this 24-to-72-hour window for acute presentations. That clinician will determine whether same-day referral to a board-certified orthopedic surgeon is warranted. Bring a description of exactly when symptoms began, which motions provoke them, and what the strength loss feels like in functional terms (can you lift a gallon of milk, can you reach a shelf, can you put on a jacket).
How a Torn Rotator Cuff Is Diagnosed Clinically
A torn rotator cuff is diagnosed through a combination of physical examination tests that isolate individual tendon function and imaging studies, primarily magnetic resonance imaging (MRI) or musculoskeletal ultrasound, that directly visualize the tendon integrity.
The physical examination comes first. Experienced orthopedic surgeons and sports medicine physicians can predict the likely involved tendon with high accuracy using a structured battery of clinical tests before any imaging is ordered. A 2016 systematic review in the American Journal of Sports Medicine found that the combination of the Neer sign, Hawkins-Kennedy test, and painful arc has pooled sensitivity of approximately 72 percent and specificity of 66 percent for identifying rotator cuff tears, with individual test combinations improving accuracy substantially.
Named clinical tests and what they assess:
| Clinical Test | Tendon Targeted | What Is Assessed | Clinical Significance When Positive |
|---|---|---|---|
| Jobe (empty can) test | Supraspinatus | Arm elevation against resistance in scapular plane with internal rotation | Supraspinatus tear or impingement |
| Drop arm test | Supraspinatus | Ability to sustain 90-degree abduction after arm is passively elevated | High specificity (97%) for full-thickness supraspinatus tear |
| Neer impingement sign | Supraspinatus, subacromial bursa | Passive forward flexion provokes impingement pain | Subacromial impingement, bursal inflammation |
| Hawkins-Kennedy test | Supraspinatus, subacromial bursa | Internal rotation with 90-degree forward flexion compresses subacromial space | Impingement syndrome, supraspinatus pathology |
| Lift-off test | Subscapularis | Ability to push hand off low back | Subscapularis tear |
| External rotation lag sign | Infraspinatus | Inability to maintain arm in passive external rotation | Large infraspinatus or teres minor tear |
Imaging follows when the clinical examination confirms suspected rotator cuff pathology or when the diagnosis is uncertain. MRI without contrast is the standard first-line imaging study. It visualizes the tendon in multiple planes, identifies tear size, evaluates degree of tendon retraction, and assesses fatty infiltration of the rotator cuff muscles. Musculoskeletal ultrasound is a useful alternative: it is less expensive, dynamic (allows real-time tendon assessment during movement), and avoids the claustrophobia concerns of MRI, but its accuracy is highly operator-dependent.
Plain radiographs (X-rays) do not visualize tendons directly but identify secondary bony changes: superior humeral head migration, acromial spur formation, and glenohumeral joint space narrowing, all of which can suggest the chronicity and severity of rotator cuff disease.
Key Takeaway: A torn rotator cuff is most reliably diagnosed through a structured physical examination using named clinical tests combined with MRI, and a clinician can often predict the involved tendon accurately before imaging based on the specific directional weakness pattern alone.
Emergency Symptoms: When to Call 911 or Go to the ER
Certain symptoms associated with shoulder injury and rotator cuff pathology require immediate emergency evaluation. Do not wait to see if these resolve on their own.
Call 911 or go to the nearest emergency room immediately if you experience:
- Sudden complete loss of arm function following a high-energy injury such as a fall from height, a motor vehicle collision, or a violent forced arm movement. This presentation can indicate massive rotator cuff rupture combined with glenohumeral dislocation or brachial plexus injury.
- Visible shoulder deformity with the arm locked in an abnormal position, suggesting glenohumeral dislocation requiring immediate reduction.
- Severe swelling and rapid bruising spreading from the shoulder into the upper chest or axilla (armpit) after trauma. This pattern can indicate injury to the axillary artery or axillary vein, both of which are vascular emergencies.
- Complete loss of sensation or movement in the entire arm following shoulder trauma. This presentation requires emergency evaluation for brachial plexus avulsion or vascular injury.
- Fever exceeding 38.5 degrees Celsius (101.3 degrees Fahrenheit) with severe, rapidly worsening shoulder pain that is not explained by known trauma. This combination can indicate septic arthritis of the glenohumeral joint, which requires emergency joint aspiration and antibiotics to prevent permanent joint destruction.
- Chest pain, shortness of breath, or left arm pain accompanying shoulder symptoms in adults over 45. These symptoms in combination can represent acute myocardial infarction presenting atypically with shoulder pain, not a rotator cuff problem.
These presentations can indicate a vascular emergency, a septic joint, an acute brachial plexus injury, or a cardiac event and require emergency medical assessment, not an urgent care appointment or a phone call.
Frequently Asked Questions About Rotator Cuff Tear Symptoms
Can you still move your arm with a torn rotator cuff?
Many people with a torn rotator cuff can still move their arm, particularly if the tear is partial or involves only one of the four tendons.
Full-thickness tears of the supraspinatus can still allow forward elevation if the deltoid compensates, though abduction strength is measurably reduced.
A massive tear involving multiple tendons often produces pseudoparalysis, a near-complete inability to elevate the arm against gravity despite intact neurological function.
What does a torn rotator cuff feel like compared to a regular shoulder strain?
A rotator cuff tear typically produces a deep ache inside the joint rather than the surface muscle soreness of a standard strain.
Pain that is specifically worse during arm elevation between 60 and 120 degrees (the painful arc), accompanied by directional weakness and night pain, is more consistent with rotator cuff pathology than muscle strain.
Muscle strains typically resolve within one to three weeks with rest; rotator cuff tear symptoms persist and often progress without targeted evaluation and treatment.
How do I know if my rotator cuff is partially or fully torn?
You cannot reliably determine this at home. A partial tear often allows near-normal arm elevation with mild weakness, while a full-thickness tear produces a more pronounced and consistent strength deficit.
The drop arm test (inability to hold the arm at 90-degree abduction after passive elevation) has approximately 97 percent specificity for full-thickness supraspinatus tears, according to research in the Journal of Shoulder and Elbow Surgery.
Only clinical examination combined with MRI or musculoskeletal ultrasound can confirm tear depth, extent, and which tendon is involved.
Can a torn rotator cuff heal on its own without surgery?
Partial-thickness rotator cuff tears, particularly smaller tears in younger adults, can stabilize or improve with structured physical therapy, activity modification, and time.
Full-thickness tears do not regenerate tendon continuity on their own; without surgical repair, they typically enlarge over time and accumulate secondary muscle fatty infiltration.
According to the American Academy of Orthopaedic Surgeons, conservative management (physical therapy, anti-inflammatory treatment) is appropriate initial treatment for many rotator cuff tears, but large full-thickness tears in active, younger patients generally benefit from surgical repair to restore full function.
What are the first signs of a rotator cuff tear?
The first signs of a rotator cuff tear are typically a dull ache at the outer shoulder that appears after overhead activity and resolves with rest, followed by progressive discomfort that lingers longer after each provocative activity.
Mild difficulty lifting the arm to shoulder height, subtle weakness when reaching overhead, and the first episodes of night pain on the affected side are early warning signs that should not be dismissed as simple muscle soreness.
Early evaluation by a primary care physician or sports medicine physician leads to better treatment outcomes because smaller partial tears respond well to conservative care before they enlarge.
What type of doctor should I see for rotator cuff tear symptoms?
A primary care physician or sports medicine physician is an appropriate first contact for rotator cuff tear symptoms that have developed gradually over weeks.
If the primary care evaluation suggests a significant tear, or if imaging confirms a full-thickness or large partial tear, referral to a board-certified orthopedic surgeon with shoulder subspecialty experience is the appropriate next step.
For acute presentations after trauma with sudden complete loss of shoulder function, go directly to the emergency room; do not wait for an outpatient appointment.
Closing
Rotator cuff tear symptoms follow a clinically recognizable pattern once you understand the anatomy behind them. Pain localized to the outer shoulder, directional arm weakness that maps to specific tendons, night pain driven by subacromial space compression in lateral sleep positions, and a progressive course that worsens without evaluation are the hallmarks. The four-tendon architecture of the rotator cuff means that each symptom is mechanistically linked to a specific structure, and knowing which symptom points to which tendon is genuinely useful when you are trying to describe your experience to a clinician.
If you have had shoulder pain or weakness for more than four to six weeks without improvement, or if your symptoms began suddenly after a fall or forceful movement, contact a primary care physician or a sports medicine physician. Ask specifically about clinical examination of rotator cuff integrity and whether imaging is indicated. In adults over 60 with new functional weakness, do not wait for symptoms to become severe before seeking evaluation. The window for effective treatment, surgical or conservative, narrows significantly as tears enlarge and secondary muscle changes develop.
You are now equipped to describe your symptoms with clinical precision, understand what the physical findings mean, and know exactly when your situation calls for urgent versus scheduled care.