What Causes Tonsil Stones? The Real Reasons Explained
Tonsil stones form when organic debris, anaerobic bacteria, and salivary minerals accumulate inside the deep crevices of your palatine tonsils, gradually hardening into calcified lumps called tonsilloliths. Understanding what causes tonsil stones means understanding the specific anatomy of your tonsils and the bacterial and biochemical processes that turn trapped debris into a calcified deposit.
According to a review published in the International Journal of Otolaryngology, tonsilloliths are found in roughly 10% of the general population, though many people carry small stones without ever noticing them. They are far more common than most people realize, and in people with enlarged tonsils or a history of chronic throat infections, that prevalence rises considerably.
This article breaks down every named causal mechanism behind tonsil stone formation: the anatomy that makes it possible, the bacteria that drive the process, the specific biochemical steps that produce calcification, and the lifestyle and medical factors that increase your risk. You’ll also find specific guidance on when symptoms warrant evaluation by a primary care physician or an otolaryngologist (ear, nose, and throat specialist).
What Causes Tonsil Stones
Tonsil stones form when organic material trapped inside the crevices of the palatine tonsils combines with bacteria and undergoes a process of calcification, producing hard, whitish-yellow deposits ranging from less than one millimeter to several centimeters in size.
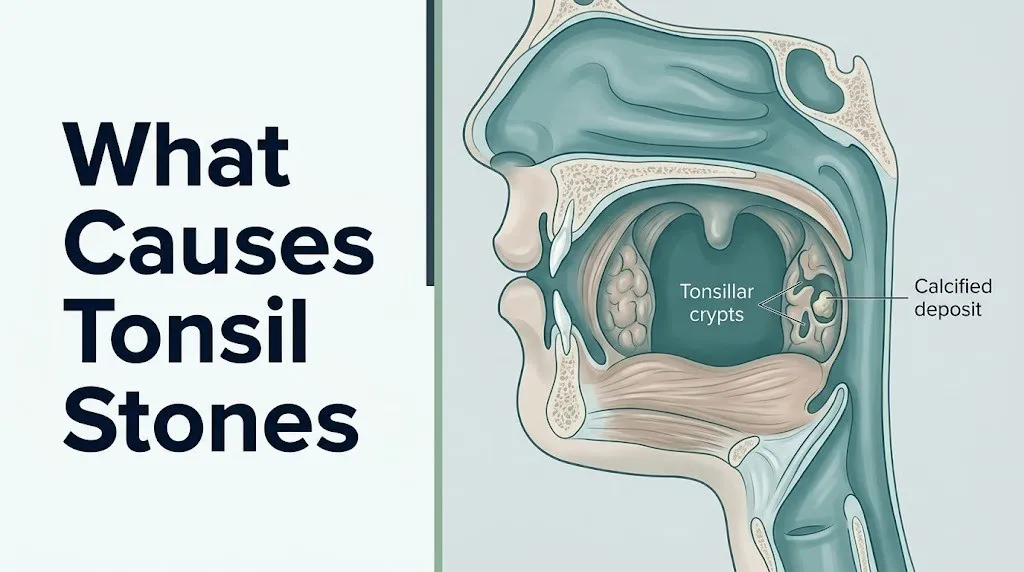
The core mechanism has three sequential steps. First, debris accumulates inside the tonsillar crypts, the narrow pockets that cover the surface of the tonsils. This debris includes food particles, dead skin cells shed from the lining of the throat, mucus, and dead immune cells. Second, anaerobic bacteria colonize this debris and form a structured community called a biofilm, consuming available oxygen and creating a sealed, oxygen-poor microenvironment. Third, salivary minerals, primarily calcium and phosphate, precipitate onto the debris matrix in this altered chemical environment, progressively mineralizing the organic material into a stone.
This is not a random process. It requires the specific structural conditions that the tonsillar crypt provides: depth, poor drainage, warm temperature, and constant proximity to both oral bacteria and saliva. Think of it like sediment building up inside a narrow pipe that rarely gets flushed. The debris accumulates because the geometry of the crypt prevents natural clearance.
Causes vary in frequency and significance:
| Cause | Mechanism | Frequency |
|---|---|---|
| Tonsillar crypt accumulation of organic debris | Debris trapping by crypt architecture | Very common: primary cause in all cases |
| Anaerobic bacterial biofilm formation | Oxygen-poor microenvironment enabling calcification | Common: present in all tonsil stones studied |
| Poor oral hygiene | Increased oral bacterial load colonizing crypts | Common modifying factor |
| Dry mouth (xerostomia) | Reduced salivary flow impairing crypt clearance | Common in medication users and dehydrated individuals |
| Chronic post-nasal drip | Mucus accumulation providing extra substrate in crypts | Common in allergy and sinus disease patients |
| Gastroesophageal reflux disease (GERD) | Acid exposure altering oropharyngeal mucosal environment | Moderate: emerging contributing factor |
| Chronic or recurrent tonsillitis | Scarring and enlargement of crypts | Common in patients with tonsillitis history |
Individual variation is immediately relevant here. People who have never had tonsillitis but have deep crypt anatomy from birth are just as susceptible as people with a history of throat infections. The anatomy sets the stage; the bacteria and lifestyle factors determine how quickly the stone forms.
What Are Tonsil Stones Made Of
Tonsil stones are composed primarily of calcium hydroxyapatite and calcium carbonate crystals embedded in a matrix of organic material including desquamated squamous epithelial cells, dead white blood cells, mucin glycoproteins, and food particles.
Laboratory analysis of excised tonsilloliths, reported in the Journal of Oral and Maxillofacial Surgery, consistently identifies calcium and phosphate as the dominant mineral components. This is the same calcium-phosphate compound that forms tooth enamel and bone, though the route to its formation in tonsil crypts is entirely different. In teeth, calcium hydroxyapatite is deposited by specialized cells called ameloblasts under precise biological control. In tonsil crypts, it forms opportunistically through the chemical interaction between bacterial metabolic activity and salivary mineral concentration.
The organic component of a tonsil stone includes a mix of material types:
- Desquamated squamous epithelial cells shed from the tonsillar surface epithelium and the surrounding oropharyngeal mucosa
- Dead neutrophils and other immune cells that have migrated to the tonsil surface during local immune responses
- Mucin glycoproteins from saliva and post-nasal drip mucus
- Food particles, particularly protein-rich fragments from meat, dairy, and starchy foods
- Bacterial cell debris and extracellular matrix components from the biofilm
The mineral content increases over time as long as the stone remains lodged in the crypt. Small, newly formed stones may be mostly soft organic material. Older or larger stones have a harder mineral shell surrounding an organic core, which explains why some tonsil stones crumble when removed and others are firm enough to resist compression.
People taking medications that reduce salivary flow, including antihistamines, tricyclic antidepressants, and certain antihypertensive agents, may develop stones with altered mineral composition because changes in salivary calcium concentration affect the rate of mineral precipitation.
Tonsil Crypt Anatomy and Stone Formation
The palatine tonsils are paired secondary lymphoid organs located in the tonsillar fossae on either side of the oropharynx, positioned between the anterior palatoglossal arch and the posterior palatopharyngeal arch. Their surface is not smooth. It is deeply invaginated by tonsillar crypts, narrow channels lined with stratified squamous epithelium that extend down into the lymphoid tissue of the tonsil body.
Each palatine tonsil contains between 10 and 30 crypts. These crypts are not incidental. They are a functional part of the tonsil’s immune surveillance role, designed to maximize surface area contact between inhaled and ingested antigens and the underlying lymphoid follicles. The reticular epithelium at the base of each crypt actively samples bacteria and particles from the oral environment and presents them to B lymphocytes and T lymphocytes within the adjacent germinal centers.
The problem is structural. The crypt is a narrow, deep, blind-ended channel with limited natural drainage. Debris enters easily, carried by air and saliva. Getting debris back out requires strong salivary flow, effective swallowing mechanics, and crypts that stay relatively shallow. When any of these factors fails, the crypt functions less like an immune checkpoint and more like a biological trap.
Think of the crypt like a narrow coin slot that faces upward. Things fall in easily. Getting them out requires something actively flushing them out, which the tonsil’s own drainage mechanism does not do efficiently when crypts are deep or scarred.
Adolescents are at particularly high risk during the years of lymphoid hyperplasia, the developmental phase when the palatine tonsils enlarge in response to the immune system’s active antigen training. Enlarged tonsils have deeper, wider, and more numerous crypts, creating more trapping surface area. As the lymphoid tissue naturally involutes after adolescence, tonsil size decreases and stone formation risk typically decreases with it in people without additional risk factors.
Bacteria That Cause Tonsil Stones
Anaerobic bacteria are the biological engine of tonsil stone formation, and specific named species drive both the creation of the biofilm matrix and the chemical environment that enables calcification.
A 2020 review published in the Journal of Oral Biosciences identified Fusobacterium nucleatum, Prevotella melaninogenica, Porphyromonas gingivalis, and Actinomyces israelii as the most consistently recovered anaerobic species from tonsillolith cultures. These organisms thrive in oxygen-depleted environments and are the same species implicated in periodontitis (gum disease), which helps explain why people with poor gum health tend to have higher rates of tonsil stone formation.
These bacteria form a biofilm: a structured, community-based growth mode in which bacteria adhere to the organic debris surface, produce an extracellular polysaccharide matrix, and establish a three-dimensional architecture. Biofilm formation is relevant to tonsil stone development for two reasons.
First, the biofilm’s extracellular matrix acts as a physical scaffold that traps additional debris and prevents salivary clearance. Second, the metabolic activity of the bacteria within the biofilm creates the specific chemical microenvironment (anaerobic, acidic at the biofilm interior, with localized alkaline zones at the biofilm-saliva interface) in which calcium-phosphate precipitation occurs.
Key bacterial roles in tonsil stone development:
- Fusobacterium nucleatum: Gram-negative anaerobe; produces hydrogen sulfide and methyl mercaptan; central structural member of the tonsil biofilm architecture
- Prevotella melaninogenica: Gram-negative pigmented anaerobe; degrades mucin glycoproteins, releasing amino acid substrates that other anaerobes catabolize into VSC
- Porphyromonas gingivalis: Gram-negative anaerobe; known periodontal pathogen; produces a range of proteolytic enzymes that degrade host tissue proteins within the crypt
- Actinomyces israelii: Gram-positive filamentous anaerobe; forms the structural core of many tonsillolith biofilms; associated with particularly hard, branching stone morphology
People who have recently completed antibiotic courses may notice a temporary reduction in tonsil stone formation, which reflects the disruption of the anaerobic biofilm community. However, because biofilms rapidly re-establish from residual bacteria, this effect is typically short-lived.
Key Takeaway: Tonsil stones are not simply trapped food. They are the end product of a specific biological process driven by anaerobic bacteria that build structured biofilms inside tonsillar crypts, setting up the chemical conditions for calcium-phosphate mineralization.
Tonsil Stone Calcification Process
Tonsil stone calcification occurs through the precipitation of calcium hydroxyapatite and calcium carbonate onto an organic debris scaffold within the tonsillar crypt, driven by the interaction between salivary mineral concentration and the pH microenvironment created by anaerobic bacterial metabolism.
Saliva is normally supersaturated with calcium and phosphate ions relative to most tissues. This saturation is physiologically important for tooth enamel remineralization. Inside the tonsillar crypt, however, this same supersaturation becomes the raw material for stone formation.
The precipitation process works like this:
- Organic debris accumulates inside the crypt and is colonized by anaerobic bacteria that form a biofilm
- Bacterial catabolism of proteins and amino acids generates ammonia and other alkaline metabolites at the biofilm-saliva interface, locally elevating pH in that specific microzone
- At elevated pH, salivary calcium and phosphate ions are more prone to precipitation rather than remaining in solution
- Calcium phosphate crystals begin forming on the organic matrix surface, specifically at the alkaline interface
- Over time, calcium carbonate adds a second mineral layer as dissolved carbon dioxide reacts with salivary calcium
- The stone grows concentrically, with new mineral layers added as long as the debris remains lodged and the bacteria remain active
The National Institute of Dental and Craniofacial Research (NIDCR) research into salivary biochemistry confirms that salivary calcium concentration varies significantly between individuals, which partly explains why some people form stones more readily than others under identical oral hygiene conditions.
People with primary hyperparathyroidism, a condition causing elevated serum calcium levels, may have altered salivary calcium concentrations that accelerate tonsil stone calcification. If you develop unusually large or rapidly growing tonsil stones without an obvious hygiene or anatomical explanation, a primary care physician should evaluate your serum calcium and parathyroid hormone levels.
What Makes Tonsil Stones Smell So Bad
The sulfurous odor of tonsil stones comes from volatile sulfur compounds (VSCs), specifically hydrogen sulfide, methyl mercaptan, and dimethyl sulfide, produced by anaerobic bacteria within the tonsil stone biofilm as byproducts of amino acid catabolism.
Hydrogen sulfide smells like rotten eggs. Methyl mercaptan has a rotten-cabbage odor. Dimethyl sulfide contributes a cooked-cabbage note. Together, these three compounds account for the distinctive, often extremely strong, sulfurous smell that makes tonsil stones one of the most common oral sources of chronic halitosis (bad breath) that does not respond to brushing and mouthwash.
The biochemical pathway is specific:
- Anaerobic bacteria in the biofilm catabolize sulfur-containing amino acids, primarily cysteine and methionine, from the protein components of trapped food debris, dead cells, and mucus
- Fusobacterium nucleatum and Prevotella melaninogenica are particularly active VSC producers
- These gases diffuse out of the tonsil crypt with every exhalation, producing breath odor that originates in the throat rather than the mouth
- Standard oral hygiene targets the tongue, teeth, and gums, not the tonsillar crypts, which is why people with tonsil stone-associated halitosis often find that mouthwash provides only temporary relief
According to the Journal of Oral Biosciences 2020 review, tonsil stone-associated halitosis is frequently resistant to standard oral hygiene interventions because the VSC source is located deep within the crypt architecture, beyond the reach of brushing or rinsing.
This matters for people who have been told their breath problems are entirely dental in origin. If you have persistent halitosis despite excellent oral hygiene and no active periodontal disease, tonsil stones are a legitimate and often overlooked source. An otolaryngologist can examine the tonsillar crypts directly and determine whether stone removal resolves the halitosis.
Can Poor Oral Hygiene Cause Tonsil Stones
Poor oral hygiene does contribute to tonsil stone formation, though it is rarely the sole cause and is not required for stones to develop.
The connection is indirect but mechanistically sound. Poor oral hygiene allows the oral microbiome to shift toward dysbiosis: a state in which anaerobic, pathogenic species overgrow relative to the commensal (harmless) bacteria that normally keep them in check. When anaerobic species like Fusobacterium nucleatum and Porphyromonas gingivalis are present in higher numbers throughout the mouth, they are more readily deposited into the tonsillar crypts during swallowing, increasing the bacterial load within the crypt and accelerating biofilm formation.
Poor oral hygiene also means more food debris, more dead cells from inflamed gum tissue, and more salivary bacteria available to enter the crypt with each swallow. Each of these increases the organic substrate that provides the scaffold for calcification.
That said, people with excellent oral hygiene still develop tonsil stones if their tonsillar crypt anatomy is deep enough. The crypt structure itself is the primary anatomical risk factor. Oral hygiene is a significant modifying factor, not an independent sufficient cause.
Steps that improve oral hygiene’s effect on tonsil stone risk:
- Brush teeth twice daily for two full minutes, including the back molars adjacent to the tonsils, to reduce the bacterial concentration available to enter the crypts
- Floss once daily to remove interdental debris that, if swallowed, can contribute to crypt accumulation
- Clean the posterior tongue with a tongue scraper to reduce VSC-producing bacteria on the tongue dorsum
- Rinse with a non-alcoholic, antiseptic mouthwash after meals to reduce residual food particles in the oropharynx
- Drink adequate water throughout the day to maintain salivary flow and natural crypt flushing
- Avoid tobacco use: smoking promotes oral anaerobic dysbiosis and reduces mucociliary clearance, increasing debris accumulation in the pharynx
Children under age 10 develop tonsil stones less commonly, not because of better oral hygiene but because their tonsil crypt architecture is shallower and their salivary flow rates relative to body size are generally higher.
Does Dry Mouth Cause Tonsil Stones
Dry mouth, clinically called xerostomia, promotes tonsil stone formation by reducing the salivary flow that normally flushes debris from tonsillar crypts and by concentrating salivary calcium in a smaller volume of saliva, which can accelerate mineral precipitation.
Saliva performs two functions relevant to tonsil stone prevention. First, salivary flow mechanically flushes material out of the crypts with each swallow, the same way a slow-running tap gradually clears sediment from a drain. When flow is reduced, this clearance mechanism is impaired. Second, saliva maintains a slightly alkaline pH and a dilute concentration of calcium and phosphate ions. When salivary flow drops significantly, relative calcium concentration rises and pH may shift, both of which favor crystal precipitation.
The Mayo Clinic identifies the following as the most common causes of xerostomia:
- Antihistamines (first-generation particularly, such as diphenhydramine)
- Anticholinergic medications (including certain overactive bladder drugs and older antidepressants)
- Tricyclic antidepressants (amitriptyline, nortriptyline)
- Antihypertensive drugs (diuretics, beta-blockers, ACE inhibitors in some patients)
- Dehydration from inadequate fluid intake, fever, or exercise
- Sjögren’s syndrome (an autoimmune condition attacking salivary and lacrimal glands)
- Radiation therapy to the head and neck region, which can permanently damage salivary gland tissue
People taking multiple medications from this list, often older adults managing several chronic conditions simultaneously, are at meaningfully higher risk for tonsil stones than younger adults with normal salivary production. If you use any of these medications and have recurrent tonsil stones, discuss xerostomia management strategies with your prescribing physician.
Drinking at least 2 liters of water daily supports salivary production. Mouth breathing at night, which dries the oropharyngeal mucosa, is another underappreciated xerostomia driver that can be addressed with a nasal strip or nasal saline rinse before sleep.
Key Takeaway: Dry mouth is one of the most actionable tonsil stone causes because it is often driven by specific, identifiable medications or behaviors, meaning addressing it can produce a measurable reduction in stone formation frequency.
Does Post-Nasal Drip Cause Tonsil Stones
Post-nasal drip contributes to tonsil stone formation by delivering excess mucus into the oropharynx, where it drains across and into the tonsillar crypts, providing a dense, protein-rich substrate that anaerobic bacteria readily colonize and metabolize.
Post-nasal drip occurs when the nasal mucosa or sinuses produce more mucus than the nasal ciliary clearance mechanism can efficiently transport to the nasopharynx and swallow. The excess drips down the posterior nasopharyngeal wall, pooling on the posterior oropharyngeal and tonsillar surfaces.
Mucus is composed primarily of mucin glycoproteins, water, electrolytes, and immunoglobulins. Mucin glycoproteins are rich in sulfur-containing amino acid side chains, which is exactly the substrate that anaerobic bacteria like Prevotella melaninogenica catabolize to produce volatile sulfur compounds. Excess mucus sitting on and around the tonsils therefore contributes both to the structural debris load within the crypts and to the VSC-producing bacterial food supply.
Conditions that produce chronic post-nasal drip relevant to tonsil stone risk include:
- Chronic allergic rhinitis (persistent inflammation of the nasal mucosa driven by allergen exposure, producing excess IgE-mediated mucus secretion)
- Non-allergic rhinitis (vasomotor rhinitis, triggered by temperature changes, strong odors, or humidity shifts)
- Chronic rhinosinusitis (persistent inflammation of the sinus mucosa producing thick, bacterial-laden mucus)
- Nasal polyps (benign mucosal growths that impair drainage and increase mucus production)
- Deviated nasal septum (structural displacement that impairs nasal airflow and promotes unilateral mucus pooling)
People with seasonal allergies frequently notice that tonsil stone formation worsens during peak allergy season. This is a direct reflection of the increase in post-nasal drip volume and bacterial substrate during periods of maximal allergic nasal inflammation. Managing the underlying allergic rhinitis with appropriate antihistamines or intranasal corticosteroids, under the guidance of a primary care physician or allergist, can reduce post-nasal drip and modestly reduce tonsil stone formation rates in these individuals.
Does Acid Reflux Cause Tonsil Stones
Gastroesophageal reflux disease (GERD) contributes to tonsil stone development through two separate pathways: acid-mediated mucosal irritation that increases epithelial cell shedding in the oropharynx, and the direct deposition of gastric acid and pepsin into the oropharyngeal environment, which alters the pH and microbial balance of the tonsillar crypt microenvironment.
When gastric acid refluxes past the upper esophageal sphincter into the pharynx, a condition sometimes called laryngopharyngeal reflux (LPR), it contacts the posterior oropharyngeal wall and tonsillar surfaces. The low-pH acid environment injures the stratified squamous epithelium, accelerating the shedding of surface cells into the tonsillar crypts. This increases the available organic substrate for stone formation.
Additionally, the acid exposure alters the oropharyngeal microbiome by killing acid-sensitive commensal bacteria while sparing or selecting for acid-tolerant anaerobic species. This microbial shift promotes the overgrowth of exactly the biofilm-forming anaerobic bacteria associated with tonsil stone formation.
Research published in the Archives of Otolaryngology-Head and Neck Surgery found an association between LPR and tonsillar enlargement, tonsillar crypt changes, and increased rates of oropharyngeal complaints consistent with tonsil stone formation. The evidence is observational rather than from controlled trials, but the mechanistic rationale is well-grounded in oropharyngeal mucosal physiology.
People with GERD should note: acid reflux can cause throat symptoms that mimic tonsil stones, including a persistent sensation of something stuck in the throat (globus pharyngeus), chronic cough, and throat clearing. A primary care physician or gastroenterologist can distinguish GERD-related throat symptoms from tonsil stone-related symptoms through a clinical history, possibly supplemented by a 24-hour pH impedance study or a direct oropharyngeal examination.
Effective GERD management, through dietary modification, positional changes, and physician-supervised acid suppression therapy where appropriate, may reduce oropharyngeal epithelial injury and modestly decrease tonsil stone frequency in affected individuals.
Key Takeaway: Three of the most common modifiable causes of tonsil stones, dry mouth, post-nasal drip, and acid reflux, are medical conditions that your primary care physician can evaluate and manage directly, which means addressing them may reduce stone formation without requiring any throat-specific intervention.
What Foods Cause Tonsil Stones
No specific food directly causes tonsil stones, but certain food types increase the volume of debris deposited in the tonsillar crypts and promote the oral bacterial environment that drives stone formation.
Dairy products are the most frequently associated food category. Milk, cheese, and yogurt leave calcium-rich protein residues in the oropharynx after consumption. The casein proteins in dairy products are particularly slow to clear from mucosal surfaces, providing a calcium- and protein-rich substrate in the crypts. Some individuals notice a clear relationship between dairy consumption and increased tonsil stone formation or worsening stone odor, though controlled research on this specific association is limited to clinical observation rather than randomized data.
Foods that consistently contribute to increased crypt debris load:
- Dairy products: casein proteins and calcium residues provide both mineral and organic substrate
- Starchy, crumb-producing foods: bread, crackers, and chips leave fine particulate debris that clings to the tonsillar surface and settles into crypts
- Sugary foods and drinks: sugar fuels rapid oral bacterial proliferation, shifting the microbiome toward more fermentative and anaerobic species
- Alcohol: reduces salivary flow acutely and promotes oral dysbiosis with repeated use
- Caffeinated beverages: mildly diuretic, contributing to relative dehydration and reduced salivary flow if fluid replacement is inadequate
Drinking water after every meal is a practical and evidence-consistent approach to reducing food debris accumulation in the crypts. Rinsing with saltwater after meals can further reduce the bacterial load in the posterior oropharynx.
Adolescents eating high-dairy, high-starch diets while simultaneously going through lymphoid hyperplasia face a combined structural and dietary risk that explains the frequent peak in tonsil stone complaints during the teenage years.
Tonsil Stones Risk Factors
Multiple factors increase an individual’s risk of developing tonsil stones, and they act through the same shared mechanism: increasing the debris load, the bacterial colonization, or the mineral concentration within the tonsillar crypts.
According to the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS), the following are recognized clinical risk factors for tonsillolith development:
| Risk Factor | Mechanism | Population Most Affected |
|---|---|---|
| Deep tonsillar crypt anatomy | Increased trapping surface area | All ages; anatomically determined |
| History of recurrent tonsillitis | Crypt scarring and enlargement from repeated infection | Children, adolescents, young adults |
| Lymphoid hyperplasia | Enlarged tonsils with more and deeper crypts | Adolescents aged 10 to 19 |
| Dry mouth (xerostomia) | Impaired salivary crypt clearance, concentrated minerals | Adults on multiple medications; Sjögren’s syndrome patients |
| Chronic allergic rhinitis | Increased mucus substrate in crypts | Adults and adolescents with atopic disease |
| GERD / laryngopharyngeal reflux | Mucosal injury and oropharyngeal microbiome disruption | Adults with acid reflux diagnoses |
| Poor oral hygiene | Increased oral anaerobic bacterial load | All ages |
| Tobacco use | Promotes oral anaerobic dysbiosis, reduces mucociliary clearance | Adults |
| Mouth breathing | Dry oropharyngeal environment reducing crypt clearance | Any age, particularly with nasal obstruction |
| Immunosuppression | Impaired local tonsil immune surveillance | HIV patients, transplant recipients, those on immunosuppressive medication |
People who are immunocompromised deserve specific mention. The palatine tonsil’s immune function depends on intact B and T lymphocyte populations within the tonsillar follicles. When immunosuppressive medications or conditions impair local immune surveillance, the tonsil may become a site of chronic low-grade infection rather than efficient antigen processing, which increases the cellular debris load within the crypts substantially.
Chronic Tonsillitis and Tonsil Stones Connection
Chronic and recurrent tonsillitis directly causes structural changes in the palatine tonsils that make tonsil stone formation significantly more likely, and the two conditions frequently coexist in a mutually reinforcing cycle.
Each episode of acute tonsillitis produces local inflammation, tissue swelling, and, upon resolution, a degree of fibrous scarring within the tonsillar tissue. This scar tissue distorts the normal crypt architecture. Crypts that were previously shallow and relatively self-draining become deeper, narrower, and more tortuously shaped after repeated infections. The scarred crypt is a more efficient debris trap and a less effective self-cleaning structure.
Additionally, repeated tonsillitis establishes a pattern of elevated anaerobic bacterial colonization within the crypt. Each episode introduces pathogenic bacteria into the tonsil’s immune processing environment. Bacteria that survive the immune response and antibiotic treatment may establish persistent biofilms within the scarred crypt walls, creating a chronic infection niche that is never fully cleared.
The bidirectional relationship matters clinically:
- Chronic tonsillitis causes the structural changes that promote tonsil stone formation
- Tonsil stones harboring bacteria may contribute to recurrent bouts of tonsillar inflammation, maintaining the infectious cycle
- People with both conditions frequently have a history of multiple antibiotic courses that temporarily reduce symptoms without resolving the underlying structural predisposition
The American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) guidelines on tonsillectomy consider recurrent tonsillitis with evidence of chronic tonsil stone formation as a relevant clinical factor when evaluating surgical candidacy. Tonsillectomy eliminates both conditions simultaneously, as removing the tonsils removes the crypts entirely.
Adults with persistent tonsil stones and a history of more than three to four episodes of tonsillitis annually should discuss tonsillectomy candidacy with an otolaryngologist.
What Causes Recurring Tonsil Stones
Recurring tonsil stones are driven by the same underlying anatomy and microbiology that caused the first stone, meaning the root cause has not been addressed rather than the stones themselves returning from a single event.
The most common reason tonsil stones recur is that the tonsillar crypt architecture remains unchanged after stone removal. If you remove a stone from the crypt but the crypt’s depth, shape, and bacterial colonization are unchanged, the conditions for the next stone are fully intact. The crypt will begin accumulating debris again immediately.
Specific causes of high recurrence frequency:
- Persistently deep tonsillar crypts that are anatomically irreducible without surgical intervention
- Ongoing chronic post-nasal drip that continuously deposits mucus substrate into the crypts despite stone removal
- Unmanaged GERD with persistent oropharyngeal mucosal irritation
- Chronic poor oral hygiene that maintains a high oral anaerobic bacterial load
- Xerostomia from long-term medication use that cannot be discontinued
- Incomplete stone removal, leaving debris within the crypt that seeds the next stone’s organic matrix
- Persistent low-grade tonsillar infection that maintains bacterial biofilm activity within the crypt walls even between symptomatic episodes
People who remove tonsil stones at home using cotton swabs or oral irrigators frequently report partial removal, where visible material is cleared but deeper material within the crypt remains. This partial clearance may reduce symptoms temporarily but does not eliminate the bacterial biofilm, meaning recurrence typically occurs within days to weeks.
If you have tonsil stones recurring more frequently than every two to three months, or if they are growing larger over time, an otolaryngologist can perform a full tonsillar examination, identify whether the crypt anatomy or an ongoing infection is the primary driver, and discuss options ranging from formal crypt irrigation to cryptolysis (a procedure that ablates or seals the crypt openings using laser or radiofrequency energy) or tonsillectomy.
Key Takeaway: Recurring tonsil stones almost always mean the underlying anatomical or microbial condition has not changed. Removing stones repeatedly without addressing the crypt structure, bacterial colonization, or contributing medical conditions is management of the symptom without resolution of the cause.
Who Is Most Likely to Get Tonsil Stones
Tonsil stones are most common in adolescents and young adults, in people with a history of chronic or recurrent tonsillitis, and in anyone whose tonsils have naturally deep crypt architecture, though they can occur in any adult who still has their tonsils.
Several population groups face meaningfully elevated risk:
Adolescents aged 12 to 20: The lymphoid hyperplasia that occurs during immune system development produces enlarged palatine tonsils with deeper, more numerous crypts. This is the peak age window for tonsil stone formation. The combination of enlarged tonsil anatomy, frequent upper respiratory infections during the school-age years, and dietary patterns high in dairy and starchy foods creates the maximum convergence of risk factors.
Adults with a history of chronic tonsillitis: Repeated tonsillar infections produce crypt-distorting scar tissue that increases trapping efficiency and persistent bacterial colonization, as described in the preceding section.
Adults taking xerostomia-inducing medications: Particularly relevant for adults over 40 managing multiple chronic conditions, where polypharmacy commonly includes antihistamines, antidepressants, antihypertensives, and bladder medications simultaneously.
People with chronic allergic rhinitis or chronic sinusitis: The constant post-nasal drip from these conditions provides a continuous supply of mucin substrate for the tonsillar crypts.
People with Sjögren’s syndrome: This autoimmune condition destroys salivary and lacrimal gland tissue, producing severe xerostomia that dramatically impairs the salivary flushing of tonsillar crypts. Tonsil stones are a common but underrecognized complication of Sjögren’s syndrome.
The Centers for Disease Control and Prevention reports that Sjögren’s syndrome affects an estimated 1 to 4 million Americans, with women comprising approximately 90% of cases. Given the xerostomia-mediated mechanism, tonsil stones in this population warrant otolaryngology evaluation and a discussion of salivary substitutes and enhanced oral hygiene protocols.
Biologically, males and females appear equally susceptible on a structural basis, though some clinical observations suggest women report tonsil stone-associated halitosis more frequently, possibly reflecting sex-based differences in salivary composition or in health care seeking behavior. The available data is insufficient to definitively confirm a sex-specific difference in prevalence.
How to Know If You Have Tonsil Stones
Tonsil stones produce a recognizable cluster of symptoms, though small stones are often entirely asymptomatic and discovered incidentally when a person looks in the back of their mouth with a flashlight.
The most reliable symptom cluster includes:
- White or yellowish lumps visible at the back of the throat, on or in the surface of the tonsils, ranging from pin-head size to grape size in rare cases
- Persistent bad breath (halitosis) that does not respond to brushing, flossing, or mouthwash, with a sulfurous or rotten smell that is distinct from morning breath
- A sensation of something stuck in the throat, sometimes described as a lump, pressure, or the need to constantly clear the throat
- Mild throat discomfort or soreness localized to one or both tonsil areas, particularly when swallowing
- Referred ear pain, specifically a deep ache inside the ear on the same side as the affected tonsil, caused by the shared nerve supply of the tonsil and the external auditory canal through the glossopharyngeal nerve (cranial nerve IX) and auricular branch of the vagus nerve
- A metallic or bitter taste at the back of the throat, particularly if a stone has recently dislodged
The referred ear pain is one of the most diagnostically useful symptoms because it occurs without any ear examination finding, which distinguishes it from otitis media or otitis externa. If a primary care physician finds a normal ear examination in a patient complaining of persistent ear ache on one side, examining the ipsilateral tonsil for a lodged stone is a clinically appropriate next step.
Self-examination technique:
- Stand in front of a well-lit mirror with a small flashlight or use the flashlight feature on a smartphone
- Open the mouth wide and depress the tongue slightly with a clean spoon or tongue depressor
- Direct the light toward the back of the throat, specifically at the soft tissue between the soft palate and the back wall of the throat
- Look for white, cream-colored, or yellowish material embedded in or protruding from the tonsil surface
- Do not use fingers or pointed objects to probe the tonsil surface, as this risks bleeding and can push debris deeper into the crypt
Emergency Symptoms: When to Call 911 or Go to the ER
Certain symptoms associated with tonsillar disease require immediate emergency evaluation. Do not wait to see if these resolve on their own.
Call 911 or go to the nearest emergency room immediately if you experience:
- Severe unilateral throat pain that is rapidly worsening and preventing you from swallowing even saliva
- A muffled, thick “hot potato” voice that developed suddenly alongside throat pain
- Drooling because swallowing is too painful to perform
- Difficulty opening your mouth (trismus), where the jaw feels locked or severely restricted
- Visible bulging or swelling of the soft palate on one side, which may push the uvula toward the opposite side
- Difficulty breathing or stridor (a high-pitched breathing sound)
- Fever above 39 degrees Celsius (102.2 degrees Fahrenheit) combined with any of the above symptoms
- Inability to drink fluids due to pain, with signs of dehydration (no urination for more than 8 hours, dry mouth, dizziness)
These symptoms indicate a possible peritonsillar abscess, a collection of pus between the tonsillar capsule and the superior pharyngeal constrictor muscle, which requires emergency surgical drainage and intravenous antibiotic therapy. A peritonsillar abscess can progress rapidly to airway compromise and is a life-threatening emergency if the swelling extends to compress the airway. These presentations require emergency medical assessment, not an urgent care appointment or a phone call.
When to See a Doctor for Tonsil Stones
Most small, asymptomatic tonsil stones do not require medical evaluation, but several clinical situations warrant timely assessment by a primary care physician or an otolaryngologist.
Schedule an appointment with a primary care physician if:
- Tonsil stones are causing persistent throat discomfort that has lasted more than two weeks
- You have bad breath despite good oral hygiene that has not resolved after two to three weeks
- You notice a tonsil stone that appears to be growing in size over days or weeks
- You are experiencing referred ear pain on one side without an ear infection
- Tonsil stones are recurring more frequently than every two to three months
- You cough up tonsil stones regularly and find the recurrence pattern disruptive to daily life
A primary care physician can perform a direct oropharyngeal examination, assess whether the tonsils show signs of chronic infection or significant crypt enlargement, and determine whether referral to an otolaryngologist is appropriate.
See an otolaryngologist directly (or ask your primary care physician for an expedited referral) if:
- Previous primary care evaluations have not resolved recurrent stone formation
- You are interested in discussing cryptolysis, laser cryptolysis, or tonsillectomy as definitive options
- Stones are accompanied by tonsillar asymmetry (one tonsil consistently appearing larger than the other)
- You have a history of peritonsillar abscess and are now developing recurrent stones on the same side
Tonsillar asymmetry deserves specific emphasis. A tonsil that appears persistently larger than its partner, particularly in an adult over age 40, is not automatically explained by tonsil stones. Persistent unilateral tonsillar enlargement in adults warrants examination by an otolaryngologist to exclude tonsillar neoplasm, which, while uncommon, presents in exactly this manner. An otolaryngologist will perform a thorough clinical examination and may order a computed tomography (CT) scan of the neck with contrast or a tissue biopsy if the clinical picture warrants it.
Frequently Asked Questions About Tonsil Stones
What exactly causes tonsil stones to form?
Tonsil stones form when organic debris (food particles, dead cells, mucus) becomes trapped inside the tonsillar crypts and is colonized by anaerobic bacteria that form a biofilm.
The bacteria’s metabolic activity creates the chemical conditions for salivary calcium and phosphate to precipitate onto the organic matrix, progressively mineralizing it into a calcified deposit called a tonsillolith.
The combination of deep crypt anatomy, anaerobic bacterial colonization, and salivary mineral precipitation are the three required elements for every tonsil stone.
Why do my tonsil stones keep coming back?
Tonsil stones recur because the underlying anatomical conditions inside the tonsillar crypts have not changed after stone removal.
If the crypts remain deep, the bacterial biofilm within the crypt walls is not eliminated, and any contributing factors like dry mouth, post-nasal drip, or GERD remain unmanaged, the crypt will begin producing a new stone within days to weeks.
Recurring tonsil stones that do not respond to oral hygiene improvements and management of contributing conditions should be evaluated by an otolaryngologist to discuss crypt ablation procedures or tonsillectomy.
Can tonsil stones go away on their own?
Small tonsil stones frequently dislodge and are swallowed without the person ever noticing, particularly during vigorous coughing, swallowing, or oropharyngeal muscle movement.
Larger stones lodged deeper in the crypts are less likely to self-resolve and may continue growing as long as debris accumulation and bacterial activity continue.
If a tonsil stone has been present and symptomatic for more than two to three weeks without dislodging, evaluation by a primary care physician is appropriate.
Do tonsil stones mean I have bad oral hygiene?
Tonsil stones do not exclusively indicate poor oral hygiene, as they can develop in people with excellent oral hygiene if the tonsillar crypt anatomy is sufficiently deep.
Poor oral hygiene is a contributing factor because it increases the oral anaerobic bacterial load available to colonize the crypts, but it is not a required cause.
If you have recurrent tonsil stones despite thorough oral hygiene, the primary driver is more likely your tonsil anatomy, a contributing medical condition, or medications affecting salivary flow.
What is the fastest way to get rid of tonsil stones at home?
Gentle irrigation of the tonsillar area using a Water Flosser or oral irrigator on the lowest pressure setting is generally the most effective and safest home approach for dislodging visible tonsil stones.
Gargling with warm salt water (half a teaspoon of salt in eight ounces of warm water) several times daily can help loosen smaller stones and reduce the bacterial load in the oropharynx.
Avoid using cotton swabs, toothpicks, or fingers to probe the tonsils, as this can cause bleeding, push debris deeper into the crypt, and risk introducing additional bacteria.
When should I see a doctor about tonsil stones?
See a primary care physician if tonsil stones cause persistent throat pain, bad breath lasting more than two weeks despite good oral hygiene, recurring stones more frequently than every two to three months, or ear pain on the same side as the affected tonsil.
Go to the emergency room immediately for severe unilateral throat pain with difficulty swallowing, a muffled voice, trismus (jaw restriction), or visible soft palate swelling, as these may indicate a peritonsillar abscess requiring emergency drainage.
An otolaryngologist is the appropriate specialist for patients seeking cryptolysis, laser treatment, or tonsillectomy as a long-term solution for recurrent tonsil stone formation.
Closing
Tonsil stones are not a mysterious or random event. They are the predictable result of a specific anatomical structure (deep tonsillar crypts) combined with a specific biological process (anaerobic biofilm formation and calcium-phosphate precipitation). Understanding what causes tonsil stones at this level means you can identify which factors in your specific situation are modifiable and take targeted steps rather than just treating stones as they appear.
Start with the factors most within your control: hydration, oral hygiene, management of post-nasal drip or acid reflux if those conditions apply to you, and a review of any medications that may be reducing salivary flow. These changes address the bacterial substrate and the crypt clearance mechanism directly.
If stones continue to recur despite those adjustments, or if you have persistent throat discomfort, unexplained ear pain on one side, or noticeably asymmetric tonsils, schedule an appointment with your primary care physician. They can examine the tonsils, assess for chronic infection or structural changes, and refer you to an otolaryngologist if the anatomical or clinical picture warrants it. That single appointment is the most effective step you can take once the simpler measures have been tried.